judiciary.house.gov |Today, the House Judiciary Subcommittee on the Administrative
State, Regulatory Reform, and Antitrust, led by Chairman Thomas Massie
(R-KY), released an interim staff report titled, "Politics, Private Interests, and the Biden Administration's Deviation from Agency Regulations in the COVID-19 Pandemic" The
report details how the Biden Administration pressured the Food and Drug
Administration (FDA) to go beyond its regulatory authority to change
its procedures, cut corners, and lower agency standards to approve the
Pfizer COVID-19 vaccine and authorize boosters. This approval enabled
the Biden Administration to mandate the COVID-19 vaccine, despite
concerns that the same vaccine was causing injury among
otherwise healthy young Americans.
"In August 2021, when the Pfizer shots received FDA licensure, and just
before the booster received EUA, the top two FDA vaccine reviewers with
decades of experience announced they were leaving the agency," said Chairman Thomas Massie (R-KY).
"During the pandemic, politics overruled science at the government
institutions entrusted with protecting public health. The FDA abandoned
its congressional directive to protect citizens from false claims and
undisclosed side effects, and instead ignored its own rules to pursue a
policy of promoting the vaccine while downplaying potential harms.
Exposing and acknowledging mistakes that were made is a necessary step
toward restoring integrity and trust in our regulatory agencies."
The
Subcommittee's investigation also revealed that the administrative
state mishandled reports of vaccine injury, despite requirements to
actively obtain, synthesize, and report feedback on the safety and
efficacy of the Emergency Use Authorization (EUA) vaccine. Two former
FDA scientists, Dr. Marion Gruber and Dr. Philip Krause, testified to
the Subcommittee that they felt pressure to cut corners on the vaccine
review, which was due to outside pressure to provide immediate approval
so that the government could mandate vaccines. Despite evidence of harms
from the EUA vaccine, the Biden Administration sought to fully approve
the Pfizer vaccine through the Biologics Licensing Application (BLA)
process.
Under the leadership of then-Acting FDA Commissioner Dr. Janet Woodcock,
a long-time FDA staffer who the Biden Administration promoted to Acting
Commissioner, and Dr. Peter Marks, head of the FDA's Center for
Biologics Evaluation and Research (CBER), the agency cut corners in its
usually rigorous BLA process to brand the Pfizer EUA vaccine as the only
fully licensed "safe and effective" COVID-19 vaccine on the market at
the time. Today, former Acting FDA Commissioner Woodcock says that, as
it relates to vaccine-related injury, she is "disappointed in
[her]self" and that the FDA did not do enough to address
vaccine-related injury.
The FDA succumbed to the Biden Administration's pressure to act beyond
its authority, which may have long-term impacts on the agency's ability
to confidently serve the American public. This poor policy by the Biden
Administration reveals many significant problems related to
accountability and good decision making in the administrative state that
warrant legislative reform.
Read the full interim staff report and appendix here.
brownstone | In the final chapters of The Wuhan Cover-Up, RFK, Jr.
focuses on several key figures in the biowarfare-industrial-complex,
including Jeremy Farrar of the Wellcome Trust (now at the WHO), Anthony
Fauci of the NIH, and Bill Gates.
RFK, Jr. uses these figures to show how the Covid pandemic emerged
from the toxic stew of ethically compromised biowarfare research
standards; military, intelligence, public health, and academic
institutions/organizations dependent on biowarfare funding; the
involvement of China and global interests in the booming business of
“pandemic preparedness and response;” and, of course, the endless
pursuit of political power and personal enrichment.
Here’s a great summary of how they all came together, through
personal and institutional greed and power-mongering, to unleash the
Covid catastrophe on the world:
The evidence suggests that instead of relentlessly protecting public
health, Farrar exploited the pandemic to promote the venal financial
agendas of his WEF [World Economic Forum] patrons, to transform Western
democracies into surveillance states, to expand his personal power and
paycheck, and to pander to high-level Chinese officials. Achieving these
objectives required Farrar to hide [Covid’s] laboratory origins, a
project in which he enlisted a cadre of his medical cartel cronies—those
who, thanks to years of funding by Fauci, Farrar, and Gates, now occupy
the highest echelons of virology in academia, the regulatory agencies,
and pharmaceutical companies.
(p. 539)
If for nothing else, I would recommend adding The Wuhan Cover-Up
to your library as an invaluable resource on leading figures,
organizations, and power brokers involved in the
biowarfare-industrial-complex.
In fact, after reading the first few chapters – the ones that go into
the history of chemical and biological warfare and the rise of the
biowarfare-industrial-complex – I paradoxically felt an enormous sense
of relief.
Finally, we have a detailed account that shows – beyond what I would
consider a reasonable doubt – that the entire Covid catastrophe was
caused, and led, by a multinational
military-intelligence-academic-pharma-tech-NGO cabal.
RFK, Jr.’s conclusion is that we should look to a future “in which
the bio-elites are held responsible for their actions, people regain
their rights, and the Constitution is restored to its intended
preeminence.”
But how do we do that?
I am afraid, based on the information in his own book, and the fact
that RFK, Jr. himself is being censored and banned so extensively from
the public square, that the solution to the problems he exposes is much
more difficult and complex than just “holding the bio-elites
responsible” which will somehow lead to people regaining their rights.
What we need to do is to shut down, or extract ourselves from, the
global biowarfare-industrial-complex that is able to convince (or
coerce?) our governments into declaring states of emergency over
supposed pandemic threats, and then curtail civil rights and impose
massive surveillance, censorship, and propaganda that would not be
permitted in non-emergency situations. Not to mention garnering enormous
wealth while forcing the world’s population to accept novel, untested, and potentially lethal medical “countermeasures.”
The Wuhan Cover-Up does a better job than any other book or
article I have read at exposing the trends, forces, and institutions
that brought us the Covid catastrophe – with hundreds of pages of notes
and references. What’s frightening is that the enormity of the problem
is beyond the scope of the book, not just to solve, but even to fully
acknowledge.
attorneycox | The
“they” is our government (federal and state). The “we” is you and me,
and the other 300+ million Americans across our country.
Alas,
here we are, entering the final quarter of 2023, and we have the United
States government, and many state governments (including New York’s
former Governor Andrew Cuomo, current left-wing Governor Kathy Hochul, and the super-majority Dem legislature) proclaiming for all to hear that they did not force anyone to do anything detrimental these past 3.5 years. UNBELIEVABLE!
Did you hear this? They are actually saying with straight faces that
they didn’t force you to wear a mask, or lockdown and shutter your
businesses, or choose between taking an experimental drug or losing your
job… Nope! They did none of that. And you - well, you are flat out crazy if you think they did. You are lying. You are exaggerating and totally overreacting.
Unfortunately
for Big Brother, ooops, I mean unfortunately for our 100% reliable,
never-lies-to-us government, we have actual documents (including lawsuits),
news stories, social media posts, and videos of the government at all
levels mandating and forcing us to do all of those things, and more.
Here’s just one example of Biden himself, the “Big Guy,” mandating the
C19 shot:
Biden is not alone. No, no. His entire administration is
right there with him. His head of OSHA, Douglas Parker, is also now
lying through his teeth about the OSHA mandate that REQUIRED
(not suggested) that all employers in the entire nation with 100 or
more employees force their employees to get the C19 shot, otherwise they
had to wear a mask and test constantly for C19. (That OSHA mandate was
struck down by SCOTUS
last year because it was unconstitutional, by the way). Then there’s
the head of HHS, Xavier Becerra, saying there was never a mask mandate.
What?! Another blatant lie.
Please take the 2 minutes to watch this Congressman Kevin Kiley clip.
You truly won’t believe your ears with the bullsh#* these Biden agency
heads are spewing! As Congressman Kiley says in the video, the
government is trying to tell us that “2 + 2 doesn’t equal 4.” You don’t
get much more Orwellian than that!
Easy
answers: 1) they didn’t have the authority to do any of it (all of it
was unconstitutional) so they can’t justify and defend it now, and 2) if
they can convince you they didn’t do it before, then you won’t mind as
much when they do it again.
This should make your blood
boil. It’s particularly infuriating to those of us who were speaking
out from basically day one trying to tell people that the lockdowns, the
masking, the shots, the limited number of people at your wedding or at
your Thanksgiving table were all violations of the Constitution and our
basic human rights!
mcluhangalaxy | “We have never stopped interfering drastically with ourselves by every
technology we could latch onto,” Marshall McLuhan said in 1966. “We have
absolutely disrupted our lives over and over again. Unimpeded, the
logic of this sort of world is stasis.”
McLuhan believed deeply in man’s need to comfort his self from the
onslaught of a world that seemed hostile from birth, and while
masturbation is the act of physically imitating creation, it is in
creating false media environments that man has found the greatest
comfort for his psyche.
Were McLuhan alive today, he would perhaps take great interest in two
particular aspects of modern society. The first of these aspects is the
increasingly violent nature of our world, in both the physical world
and its various media counterparts.
“When you live out on the frontier, you have no identity, you are a
nobody, therefore you get very tough,” he said in 1977. “You have to
prove you are somebody, and so you become very violent…ordinary people
find the need for violence as they lose their identities.”
What does this say about a world where violence, both real and
imagined, increases at a rate matched only by the proliferation of new
media? I believe it says that media is responsible for a world that is
increasingly violent, but not in a manner that censoring sex and
violence is capable of curbing. The nature of media is that which it is
given by man, and we have given it the nature of removing from us our
natural selves. We relinquish aspects of our identity so that we might
take shelter in the constructs that we have created to shield us from
the harsh frontiers we encounter. At each new threshold, collective
identity is lost, and with each new loss comes an increase in our
capacity for violence.
If Marshal McLuhan had lived to see his 100th year in 2011, he might
have marveled less at our technology than at our hunger for nostalgia.
It was an area of particular interest for the author and media scholar,
who said that one result of the electronic age would be a loss of
private identity owing to the discarnate being that one becomes when
broadcast electronically. Lacking a physical body in the electronic
sphere, one’s relationship to the world around them changes.
“One of the big marks of the loss of identity is nostalgia, revivals
of clothing, dances, music and shows,” he said. “We live by the revival,
it tells us who we are, or were.”
AmericanThinker |Sociology,
which is sometimes defined as the painful and tedious explication of
the obvious, occasionally comes up with useful insights, or at least
proof that some useful insights are true. That seems to be the case with
a study by Yale sociologist Andrew Papachristos, published in the
academic journal Social Science & Medicine, and featured in the Chicago Sun-Times.
It
turns out that being arrested with someone else is the best predictor
of who will get shot in Chicago. No, not by the police, as the Al
Sharptons of the world would like to claim. Shot by another civilian, in
the epidemic of shootings that have made Chicago at some times more
dangerous than Baghdad.
If
you and another person get arrested together in Chicago, you’re both
part of a loose network of people with a high risk of getting shot in
the future, Yale University researchers say in a newly published study. Only
6 percent of the people in Chicago between 2006 and 2012 were listed on
arrest reports as co-offenders in crimes, the study says. But those
people became the victims of 70 percent of the nonfatal shootings in the
city over the same period.
The
logic is pretty simple: if you are the type of person who goes out and
commits crimes with others, you are probably connected to people who
commit crimes with some frequency. And that puts you at risk of getting
shot, because people who commit crimes sometimes shoot others who
become inconvenient, or who just get in the way.
The
study is done with social network analysis, studying who knows who and
how they interact, and drawing up networks that reveal the clustering
that results from various commonalities.
The
latest Yale University study was built on Papachristos’ previous
social-network research into murders on the West Side. He had studied
killings between 2005 and 2010 in West Garfield Park and North Lawndale.
About 70 percent of the killings occurred in what Papachristos found
was a social network of only about 1,600 people — out of a population of
about 80,000 in those neighborhoods. Inside that social network, the
risk of being killed was 30 out of 1,000. For the others in those
neighborhoods, the risk of getting murdered was less than one in 1,000.
These
statistics demonstrate the wisdom of the old adage, “Lie down with
dogs, wake up with fleas.” They also show that it is not per se that is
related to the higher incidence of violence in some black communities…
For
every 100,000 people, an average of one white person, 28 Hispanics and
113 blacks became victims of nonfatal shootings every year in Chicago
over the six-year study period.
… but rather the existence of networks of people who engage in violence and reinforce each other in patters of violent behavior.
There are some useful implications for policing in Chicago IF the race demagogues don’t start calling it profiling: Fist tap Big Don.
UMKC |An ongoing law enforcement effort to rethink strategies to reduce
violent crime in the Kansas City area has its own secret weapon: UMKC.
Chancellor Leo E. Morton serves on NoVA’s governing board, and UMKC
faculty members and graduate students are embedded in NoVA’s effort to
implement a crime-prevention approach known as “focused deterrence,”
which helps police look beyond individual criminals to the criminals’
entire social networks.
The International Association of Chiefs of Police this month called
out UMKC’s relationship with the Kansas City, Missouri, Police
Department through NoVA when it awarded the department its 2014 bronze
medal for Excellence in Law Enforcement Research Award. The award
recognizes law enforcement agencies that demonstrate excellence in
conducting and using research to improve police operations and public
safety.
UMKC became involved with NoVA at the very beginning. In 2012,
Jackson County Prosecutor Jean Peters Baker came to Ken Novak, chair of
the Criminal Justice and Criminology Department, to ask how UMKC could
help curb a rising tide of violence on Kansas City-area streets. She’d
heard about focused deterrence and its success in other cities and
wanted to try it here. It just so happened that Andrew Fox had just
taken a job as a professor in UMKC’s criminology department, and Fox
happened to have experience with focused deterrence.
What if, bear with me now, what if the phase 3 clinical trials for mRNA therapeutics conducted on billions of unsuspecting, hoodwinked and bamboozled humans, was a new kind of research done to yield a new depth and breadth of clinical data exceptionally useful toward breaking up logjams in clinical terminology as well as experimental sample size? Vaxxed vs. Unvaxxed the subject of long term gubmint surveillance now. To what end?
Nature | Recently,
advances in wearable technologies, data science and machine learning
have begun to transform evidence-based medicine, offering a tantalizing
glimpse into a future of next-generation ‘deep’ medicine. Despite
stunning advances in basic science and technology, clinical translations
in major areas of medicine are lagging. While the COVID-19 pandemic
exposed inherent systemic limitations of the clinical trial landscape,
it also spurred some positive changes, including new trial designs and a
shift toward a more patient-centric and intuitive evidence-generation
system. In this Perspective, I share my heuristic vision of the future
of clinical trials and evidence-based medicine.
Main
The
last 30 years have witnessed breathtaking, unparalleled advancements in
scientific research—from a better understanding of the pathophysiology
of basic disease processes and unraveling the cellular machinery at
atomic resolution to developing therapies that alter the course and
outcome of diseases in all areas of medicine. Moreover, exponential
gains in genomics, immunology, proteomics, metabolomics, gut
microbiomes, epigenetics and virology in parallel with big data science,
computational biology and artificial intelligence (AI) have propelled
these advances. In addition, the dawn of CRISPR–Cas9 technologies has
opened a tantalizing array of opportunities in personalized medicine.
Despite
these advances, their rapid translation from bench to bedside is
lagging in most areas of medicine and clinical research remains
outpaced. The drug development and clinical trial landscape continues to
be expensive for all stakeholders, with a very high failure rate. In
particular, the attrition rate for early-stage developmental
therapeutics is quite high, as more than two-thirds of compounds succumb
in the ‘valley of death’ between bench and bedside1,2.
To bring a drug successfully through all phases of drug development
into the clinic costs more than 1.5–2.5 billion dollars (refs. 3, 4).
This, combined with the inherent inefficiencies and deficiencies that
plague the healthcare system, is leading to a crisis in clinical
research. Therefore, innovative strategies are needed to engage patients
and generate the necessary evidence to propel new advances into the
clinic, so that they may improve public health. To achieve this,
traditional clinical research models should make way for avant-garde
ideas and trial designs.
Before the COVID-19 pandemic, the conduct
of clinical research had remained almost unchanged for 30 years and
some of the trial conduct norms and rules, although archaic, were
unquestioned. The pandemic exposed many of the inherent systemic
limitations in the conduct of trials5
and forced the clinical trial research enterprise to reevaluate all
processes—it has therefore disrupted, catalyzed and accelerated
innovation in this domain6,7. The lessons learned should help researchers to design and implement next-generation ‘patient-centric’ clinical trials.
Chronic diseases continue to impact millions of lives and cause major financial strain to society8,
but research is hampered by the fact that most of the data reside in
data silos. The subspecialization of the clinical profession has led to
silos within and among specialties; every major disease area seems to
work completely independently. However, the best clinical care is
provided in a multidisciplinary manner with all relevant information
available and accessible. Better clinical research should harness the
knowledge gained from each of the specialties to achieve a collaborative
model enabling multidisciplinary, high-quality care and continued
innovation in medicine. Because many disciplines in medicine view the
same diseases differently—for example, infectious disease specialists
view COVID-19 as a viral disease while cardiology experts view it as an
inflammatory one—cross-discipline approaches will need to respect the
approaches of other disciplines. Although a single model may not be
appropriate for all diseases, cross-disciplinary collaboration will make
the system more efficient to generate the best evidence.
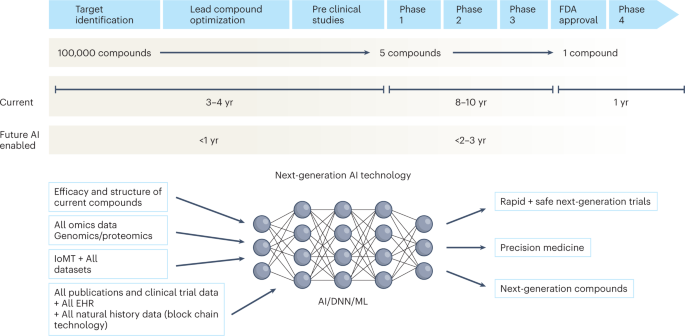
Over the
next decade, the application of machine learning, deep neural networks
and multimodal biomedical AI is poised to reinvigorate clinical research
from all angles, including drug discovery, image interpretation,
streamlining electronic health records, improving workflow and, over
time, advancing public health (Fig. 1).
In addition, innovations in wearables, sensor technology and Internet
of Medical Things (IoMT) architectures offer many opportunities (and
challenges) to acquire data9.
In this Perspective, I share my heuristic vision of the future of
clinical trials and evidence generation and deliberate on the main areas
that need improvement in the domains of clinical trial design, clinical
trial conduct and evidence generation.
Fig. 1: Timeline of drug development from the present to the future.
The
figure represents the timeline from drug discovery to first-in-human
phase 1 trials and ultimately FDA approval. Phase 4 studies occur after
FDA approval and can go on for several years. There is an urgent need to
reinvigorate clinical trials through drug discovery, interpreting
imaging, streamlining electronic health records, and improving workflow,
over time advancing public health. AI can aid in many of these aspects
in all stages of drug development. DNN, deep neural network; EHR,
electronic health records; IoMT, internet of medical things; ML, machine
learning.
Trial
design is one of the most important steps in clinical research—better
protocol designs lead to better clinical trial conduct and faster
‘go/no-go’ decisions. Moreover, losses from poorly designed, failed
trials are not only financial but also societal.
Challenges with randomized controlled trials
Randomized
controlled trials (RCTs) have been the gold standard for evidence
generation across all areas of medicine, as they allow unbiased
estimates of treatment effect without confounders. Ideally, every
medical treatment or intervention should be tested via a well-powered
and well-controlled RCT. However, conducting RCTs is not always feasible
owing to challenges in generating evidence in a timely manner, cost,
design on narrow populations precluding generalizability, ethical
barriers and the time taken to conduct these trials. By the time they
are completed and published, RCTs become quickly outdated and, in some
cases, irrelevant to the current context. In the field of cardiology
alone, 30,000 RCTs have not been completed owing to recruitment
challenges10.
Moreover, trials are being designed in isolation and within silos, with
many clinical questions remaining unanswered. Thus, traditional trial
design paradigms must adapt to contemporary rapid advances in genomics,
immunology and precision medicine11.
Brownstone | Contrary to popular belief that pharmaceutical companies drove the
COVID vaccine development programs, the US FDA’s website (FDA, 2020)
reveals that the United States Department of Defence (DoD) has been in
full control of the Covid Vaccine development program since its
beginning. The DoD has been responsible for development, manufacturing,
clinical trials, quality assurance, distribution and administration,
since that time (FDA, 2020; Rees and Latypova, 2022; KEI, 2022; Medical
Defense Consortium, 2022; Rees, 2022). The major pharmaceutical
companies have been involved as “Project Coordination Teams” effectively
performing as subcontractors to the DoD. The Chief Operating Officer
for the Warp Speed vaccine program is the US Department of Defence, and
the Chief Science Advisor is the US Department of Health and Human
Services (HHS).
The Nature of Gene-based Vaccines
The true nature of the COVID-19 ‘vaccines’ has been largely
misrepresented by mainstream media, big pharmaceutical companies and
governments and is poorly understood by the population at large.
Referring to these products as “vaccines” led most people to consider
them as relatively safe and well-researched and readily accept their
widespread use. However, they are not really vaccines – they are serious
gene-based interventions which have never been deployed widely in any
population, especially never to healthy individuals including children,
infants and pregnant women. In this sense they should be considered
experimental.
COVID-19 ‘vaccines’ fall into a special class of therapeutic agents
under the US FDA Office of Cellular, Tissue and Gene Therapies’ defined
as “gene therapy products,” which involve “introducing a new or modified
gene into the body to help treat a disease” (FDA, 2018). Heretofore,
use of gene therapy products has been limited to the treatment of
usually rare, serious and debilitating disease or genetic conditions.
They have potential to cause permanent intergenerational genetic damage,
cancer and interfere with reproductive capacity.
The FDA and other drug regulatory agencies have specific rules and
guidelines to direct manufacturers in development and testing of such
products, for both preclinical (FDA, 2013) and clinical (FDA, 2015)
research. However, the FDA did not evaluate these COVID-19 “vaccines”
according to these gene therapy guidelines.
Instead, there was a concerted effort to avoid referring to them as
gene therapy products, based, in part, on the argument that the genetic
material in the COVID-19 vaccines was not intended to be incorporated
into an individual’s DNA, nor to modify gene expression. There was no
prior short-term safety information and no long-term data on which to
predict future effects. No similar therapeutic products have been
previously approved anywhere in the world. Their widespread
administration globally with no historical safety experience was an
unprecedented risk in human health.
Accelerating Development
Messenger RNA platform technology has been researched by DARPA
(Defense Advanced Projects Research Agency) since at least 2012
(McCullough, 2022). In early 2020, in the panic to develop the COVID-19
vaccines, certain critical research and development procedures were
omitted, bypassed, curtailed, or not done in a logical sequential
manner, or to established laboratory or manufacturing standards.
Although the spike protein is the active drug and is directly
responsible for the immune response, its pharmacology and toxicology
have not been studied in animals or in humans as would normally have
been required.
Other notable deficiencies include lack of critical research on
carcinogenicity, mutagenicity, genotoxicity and reproductive toxicology
in appropriate animal species. In particular, the potential for reverse
transcription of mRNA genetic material into an individual’s DNA was not
investigated. Furthermore, scale-up manufacturing was premature and
lacked adequate quality control to ensure that product made in large
batches is the same as made in smaller batches.
Without such research, the potency, mRNA integrity, presence of
contaminants and stability of the “vaccines” cannot be guaranteed. Such
oversights are directly responsible for the failure to predict the
serious adverse drug reactions and mortality which have now been
reported in association with these vaccines.
To mitigate risk, the plan in vaccine development was to use multiple
technologies, multiple facilities and redundancy. Leverage of existing
facilities would also take place. In the interest of expediency, the
plan was to avoid using traditional pathways from early development to
large-scale production. Avoidance of quality standards and guidelines
such as Good Manufacturing Practice and Good Laboratory Practice
guidelines was necessary to speed development, and conventional New Drug
Application (NDA) and Biologics License Application (BLA) approvals
were bypassed.
Instead, the process moved rapidly using compressed timelines and
overlapping stages of development towards Emergency Use Authorization
(EUA). Scale-up and large volume manufacturing was planned in parallel
with, instead of before, clinical trials which, again, may have
contravened accepted codes of Good Manufacturing Practices. These
approaches were probably a recipe for potential disaster. (Latypova,
2022; Watt and Latypova, 2022).
newstarget | Three doctors in the armed forces have decided to blow the lid
on the United States military’s open deception concerning the negative
outcome of Wuhan coronavirus (Covid-19) “vaccination” on American
troops.
According to the three whistleblowers, medical billing code data
captured by the Defense Medical Epidemiology Database (DMED), which is
run by the Department of Defense (DoD), shows that rates of miscarriage,
myocarditis, cancer, Bell’s palsy, female infertility, and many other
health conditions are up big time.
Cancer rates are particularly concerning, they say, as the normal
average number of new cases per year is about 38,700, based on the time
period from 2016-2020. In 2021 after Operation Warp Speed was launched,
however, the number of new cancer cases that year rose to 114,645.
The Armed Forces Health Surveillance Branch (AFHSB) runs the DMED,
which it describes as a “web-based tool to remotely query de-identified
active component personnel and medical event data contained within the
Defense Medical Surveillance System (DMSS).”
“The database contains every International Classification of Diseases
(ICD) medical billing code for all medical diagnoses submitted by the
military for medical insurance billing,” reports explain. (Related:
Remember at the launch of Operation Warp Speed when Dr. Sara Beltrán
Ponce, MD, suffered a horrific miscarriage right after getting jabbed for the Chinese Flu?)
Neurological issues up 1,000% in military following Operation Warp Speed
The three military whistleblowers in question are Samuel Sigoloff,
Peter Chambers, and Theresa Long. Attorney Thomas Renz issued sworn
statements from these three to the courts as part of a major lawsuit.
During the first 10 months of 2021, Renz says, miscarriages alone
rose by 300 percent in the military. His hope is that the suit will lead
to an end for covid jab mandates in the military.
Sen. Ron Johnson (R-Wisc.) is also involved, having recently hosted
“COVID-19: A Second Opinion,” a livestreamed discussion panel featuring
numerous world-renowned doctors and medical experts who offered a much
different take on the scamdemic and how the government handled it.
On February 1 of this year, Johnson wrote a letter to U.S. Secretary
of Defense Lloyd Austin. In it were the findings from a roundtable on
covid jab injuries and deaths, including data showing a 10-fold increase
in neurological issues post-Operation Warp Speed.
Johnson also revealed the following increases in other health
conditions following the mandate of covid injections in the military:
Hypertension: 2,181 percent increase
Nervous system disorders: 1,048 percent increase
Malignant neoplasms of esophagus: 894 percent increase
Multiple sclerosis: 680 percent increase
Malignant neoplasms of digestive organs: 624 percent increase
Guillain-Barre syndrome: 551 percent increase
Breast cancer: 487 percent increase
Demyelinating: 487 percent increase
Malignant neoplasms of thyroid and other endocrine glands: 474 percent increase
Female infertility: 472 percent increase
Pulmonary embolism: 468 percent increase
Migraines: 452 percent increase
Ovarian dysfunction: 437 percent increase
Testicular cancer: 369 percent increase
Tachycardia: 302 percent increase
Between the years of 2016 and 2020, there were 1,499 codes for
miscarriage reported each year. From January through October 2021 – not
even a full year – there were an astounding 4,182 miscarriages logged
into the system.
Throughout October, there have been an average of 1,564 extra deaths
per week, compared with a weekly average of just 315 in 2020 and 1,322
in 2021.
Latest figures from the Office for National Statistics (ONS) showed
that in the week ending Oct 21, there were 1,714 excess deaths in
England and Wales, of which only 469 were due to Covid - just 27 per
cent of the total.
It is 16.8 per cent higher than normal. Deaths are also running
higher than the five-year pre-Covid October average from 2015 to 2019,
figures showed.
Health experts have warned that some of the unexplained deaths are being caused by collateral damage from the pandemic, when operations and treatments were cancelled or delayed as the health service concentrated on Covid.
The Government’s “stay at home, protect the NHS” message also left many people who needed medical treatment unwilling to bother the health service, or afraid they would catch coronavirus if they went into hospital.
The NHS is also struggling from long-term staffing issues and current shortages because of coronavirus, leading to record waits for ambulances, treatment and surgery.
Dr Charles Levinson, of the private GP service DoctorCall, which has
seen a rise in patients presenting with advanced conditions, said: “What
is driving the excess death crisis? In my view, delays in
diagnosis/treatment now and throughout the pandemic.
dailymail | Joe Biden has been re-infected with COVID
after taking an anti-viral drug that leaves patients running a 40 per
cent risk of flare-up of the virus shortly afterwards.
Taking
Paxlovid leaves COVID sufferers in danger of testing positive for the
virus again very quickly after clearing their initial infection.
When Paxlovid came to market in December 2021, studies from Pfizer indicated
that only 1-2 percent of patients who took the drug tested positive for
Covid again shortly after finishing their dosage.
But
other experts say the rapid reinfection rate is closer to 40 per cent,
and that Paxlovid can cause this issue by suppressing patients' immune
systems too early, meaning their own bodies are unable to get a handle
on COVID.
Dr. Jonathan Reiner, a
prominent cardiologist and professor of medicine and surgery at George
Washington University Hospital tweeted: 'I think this was predictable.'
He
continued: 'The prior data suggesting 'rebound' Paxlovid positivity in
the low single digits is outdates and with BA.5 is likely 20-40% or even
higher.'
In a memo released by the
White House, Dr. Kevin O'Connor said that the president will continue to
isolate, just like he did when he first tested positive on July 21.
Dr.
O'Connor also said that the president would not be prescribed Paxlovid
again. The president's doctor earlier noted that it was likely that the
president was infected with the BA.5 variant.
In June, a Mayo Clinic study showed that
five percent of adults who had taken the drug tested positive again for
Covid within 30 days, according to the New York Times.
The majority of those who experienced rebound symptoms occur within two to eight days.
Some experts have said that the current
treatment cycle of taking three pills twice a day for five days is too
short a time period to clear Covid from the patient's body.
The conclusion of the Mayo Clinic study was that extending the time period of the course of Paxlovid was unnecessary.
The authors of the study conceded in their findings that immunocompromised people were unrepresented in the study.
Also
in June, the president's chief medical advisor, Dr. Anthony Fauci,
experienced rebound Covid-19. In his case, he did take a second round of
Paxlovid.
Dr. Ashish K. Jha, the
White House’s Covid-19 response coordinator, has denied that the
Paxlovid rebound numbers are nearly 50 percent.
The doctor maintained that the actual percentage of reinfections is 'in the single digits.'
Dr. Jha said: 'When people have rebound, they don’t end up in the hospital. They don’t end up particularly sick.'
He
added: 'Paxlovid is working really well at preventing serious illness,
rebound or no rebound, and that’s why he was offered it. And that’s why
the president took it.
amidwesterndoctor |This is a supplemental addition to my previous piece.
I would strongly encourage you to read that article before reading this
one as this one goes into more tangential and complex points that
supplement the original, but many of you may find very insightful. Many
of the concepts here also appear to apply to the COVID immunizations,
however for length considerations, I will omit most of those connections
and leave you to draw your own conclusions. All of the books I cited
here can be easily found on Amazon and often as PDFs, but I avoided
linking to them here and supporting Amazon. Lastly, as I did not want to
further delay publication, a significant number of minor edits will
occur in the next few days.
I did not expect to attract the viewership the original article received, or the follow-up by larger media outlets (Steve Kirsch’s newsletter, the Kate Daley show and mercola.com)
and am sincerely grateful for your support, and those parties in
particular in spreading this message. As I now have many readers, I
will try to produce quality content as my time permits (with work and
all), as I want it to be worth your time to read what I produce. For
the time being I will focus on interesting bits of medical history (the
next piece will be interesting lessons from the 1918 influenza I applied
to my treatment of COVID).
Additionally, since my last publication a reader notified me of a short book written in 1889 and viewable online which concisely provides evidence for many of the points covered in Dissolving Illusions,
such as the lack of efficacy from the vaccination, the diseases
associated with its administration, the distortion of data used by
government officials to claim benefit rather than harm, and false claim
it reduced death in hospitals.
To be complete and
illustrate the observed effects of the smallpox vaccines, this article
is a bit longer than the previous. I could have cited significantly
more resources, but I aimed to cover one text that was representative
from each major school of thought at the time. Its sections are as
follows:
-Introduction -General Smallpox Observations -Allopathy -Naturopathy -Homeopathy -Osteopathy -Traditional Chinese Medicine -Modern Research
igorchudov |Now, for June-July, we see that more boosters mean MORE deaths and that the association between booster rates and Covid deaths is highly statistically significant!
This is the Best “Apples-to-Apples” Comparison
Let’s
summarize. We looked at the same set of countries in Europe during
three different periods of time. During the first period, booster rates
were associated with statistically significant reductions in Covid deaths. During the second period, booster rates had no effect on Covid death rates. And during the last, third period, booster rates CONTRIBUTED to greater deaths!
The
fact that all three periods involved the same countries (except a
couple who did not report booster rates during the first period), means
that this outcome is NOT due to population-wide age or other demographic
differences. The difference between outcomes in these periods is due to
the passage of time, and changes in the interaction of boosted immune
systems with the evolving virus.
Note that my data shows something much worse than “boosters stopping to work”. Instead of merely becoming useless, like in the second period, boosters became harmful and promoted deaths in the third period.
Immune Tolerance due to Boosters
Why
is this happening? Boosters and vaccines worsening Covid outcomes is
really a topic for another article to explore possible answers.
There are certainly MANY REASONS why boosters do not work anymore. Let me touch upon just one such reason. Remember that other reasons are also important!
Jan Ashton describes the “immune phenomenon known as tolerance”.
What “tolerance” means is that repeated antigen injections end up
working like allergy shots, increasing tolerance to the antigen, which
is in this case spike protein.
Tolerance towards allergens,
like tree pollen, is a good thing. (I had allergy shots myself).
However, tolerance toward a replicating virus that damages our
cardiovascular system and immune system, is a bad thing! Tolerance also
turns affected people into walking Covid superspreaders.
Instead
of seeing the viral antigen as a sign to start a battle against the
virus, the immune system says “oh well, another spike protein injection”
and ignores it. That allows the virus to multiply unchecked and cause
immense damage by killing various cells and hurting our cardiovascular
systems and more. The infected person feels less fever and less
disturbance than they would feel from a robust immune reaction, so the
illness feels “milder”, but this is actually a bad thing because the
virus multiplies unopposed.
expose-news | Dr. Nathan Wolfe was a founding citizen of Ghislaine Maxwell’s
TerraMar Project; a member of the Edge Foundation; a self-proclaimed
“virus hunter” whose area of research is zoonotic diseases with a
special focus on bats; with links to the Wuhan Institute of Virology and
EcoHealth Alliance; who previously bungled epidemic responses while
selling pandemic insurance; whose company Metabiota which is funded by
Rosemont Seneca, Google, The Skoll Foundation, among others, was awarded
a sub-contract with the US Military’s DTRA program for work in
Ukrainian biolabs.
A few days before the end of March
Russian Foreign Ministry spokeswoman Marija Zakharova published a
timeline of US-Ukraine bioresearch headed “BioBiden.” Of the 23
timeline points she listed, Nathan Wolfe or organisations associated
with him – Metabiota and Global Viral – were explicitly mentioned in 8
of them:
2007 – US DoD employee Nathan Wolfe founded Global Viral
Forecasting Institute (subsequently – Global Viral), a biomedical
company. The mission stated in the charter is non-commercial study of
transborder infections, including in China.
2014 – Metabiota, a
private commercial organisation specialising in the study of pandemic
risks is detached from Global Viral. Neil Callahan and John DeLoche,
employees of Hunter Biden’s company Rosemont Seneca Partners are
appointed to the board of Metabiota. Global Viral and Metabiota begin to
get funding from the US Department of Defence.
2014 – Metabiota
shows interest in Ukraine and invites Hunter Biden to “assert Ukraine’s
cultural & economic independence from Russia”.
2014 – Metabiota and Burisma Holdings begin cooperation on an unnamed “science project in Ukraine”.
2014
– Metabiota, Global Viral and Black & Veatch Special Projects begin
full-fledged cooperation within the US DoD programmes.
2014-2016 – Implementation of Metabiota and US DoD contracts, including a $300,000 project in Ukraine.
2016 – former US Assistant Secretary for Defence Andrew Weber is appointed head of Metabiota’s global partnerships department.
2016
– EcoHealth Alliance, a Global Viral founder Nathan Wolfe’s structure,
is engaged in the study of bat-transmitted coronaviruses at the research
centre in a Wuhan laboratory, China.
Considering the accusation is US
political elites’ involvement in the military biological activity in
Ukraine, it perhaps indicates Moscow has identified Nathan Wolfe as a
person of interest in what Zakharova termed “this truly diabolical
plan.”
“If an alien
visited Earth, they would take some note of humans, but probably spend
most of their time trying to understand the dominant form of life on our
planet –microorganisms like bacteria and viruses.”
Nathan Wolfe, Business Continuity and The Pandemic Threat Robert A Clark (2016)
From 1999 to 2006 Wolfe conducted
research as a postdoctoral student and then as an assistant professor at
Johns Hopkins University. There he worked with American epidemiologist
Donald Burke, who suspected that the practice of hunting bushmeat in
Africa had exposed a source of HIV. Based in Cameroon, Wolfe studied the
local hunters and their hunting practices. In 2004 he and his
colleagues found that 1% of bushmeat hunters were infected with the
simian foamy virus – a virus that is closely related to HIV and carried
by nonhuman primates.
In 2006 he joined the department of
epidemiology at the University of California, Los Angeles. He began
pursuing ways to monitor, predict, and prevent animal-to-human transfer
of viruses and conducted projects in Africa and Southeast Asia. In
China, he collaborated with scientists to investigate wet markets (food
markets that sell live animals) as a source of zoonoses (diseases from
wild animals).
thesaker.is | The Ministry of Defence of the Russian Federation
continues analysing the military-biological activity of the USA and its
allies in Ukraine and other regions of the world in view of new
information received at the liberated territories
and at the branch offices of the Defence Threat Reduction Agency (DTRA)
that form a unified information network.
We have previously stated that the Ukrainian
project of the Pentagon do not meet the pertinent healthcare problems of
Ukraine, while their implementation has not led to any improvement of
the sanitary-epidemiological situation.
The special military operation has led to forming the final report on DTRA activity dated from 2005 to 2016.
The document contains the data on evaluation of
healthcare, veterinary and biosecurity system efficiency prepared by a
group of U.S. experts in 2016.
This report is a concept document designed for
further planification of military-biological activity of the Pentagon in
Ukraine that contains conclusions on implementation of the programme
guidelines.
Despite the more than 10-year-long period of
cooperation in the alleged '...reduction of biological threats...', the
experts have stated:
'...There is no legislation on the control of
highly dangerous pathogens in the country, there are significant
deficiencies in biosafety... The current state of resources makes it
impossible for laboratories to respond effectively to public
health emergencies...'
The document emphasises that '...over the past five
years, Ukraine has shown no progress in implementing international
health regulations of the World Health Organisation'.
The report pays particular attention to
non-compliance with biosafety requirements when working and storing
microbial collections.
It has been stated '...that most facilities are
characterised by numerous gross violations, such as unlocked fencing
systems, unlatching windows, broken or inactive pathogen restriction
systems, lack of alarm systems...' The results of
the review conclude that there is no system for protecting dangerous
pathogens in Ukraine.
At the same time, the activities of the Defence
Threat Reduction Agency (DTRA) have been assessed positively: the
organisation has managed to bring the national collection of
microorganisms to the United States, to organise biological assessment
work and to implement projects to study particularly dangerous and
economically significant infections that could cause a worsening
(changing) epidemic situation.
The report makes the case for continuing this work on behalf of the Pentagon that has cost more than $250 million since 2005.
The document is annexed with ambiguous comments
about the sponsors and implementers of the Biological Threat Reduction
Programme in Ukraine that have nothing to do with biosecurity issues. In
particular, the Soros Foundation is mentioned
with the notation '...contributed to the development of an open and
democratic society...'
It confirms again that the official activities of
the Pentagon in Ukraine are just a front for illegal military and
biological research.
We have repeatedly mentioned the role of U.S.
Democratic Party representatives in funding bioweapons activities in
Ukraine and the intermediary organisations that have been used for this
purpose.
I would like to refer to one of the key Pentagon contractors receiving money from Hunter Biden's investment fund, Metabiota.
The available data suggests that the company is
merely a front for internationally dubious purposes and is used by the
U.S. political elite to carry out opaque financial activities in various
parts of the world.
There is a specific example: Metabiota was involved
in the response to the Ebola epidemic in West Africa. The activities of
the company's employees have raised questions from the World Health
Organisation (WHO) in terms of their compliance
with biosafety requirements.
This is the report of the international panel of
experts from the Haemorrhagic Fever Consortium who were involved in the
fight against Ebola virus disease in Sierra Leone in 2015.
According to the document, Metabiota staff had
failed to comply with handling procedures and concealed the involvement
of Pentagon staff who were using the company as a front. The main
purpose of these activities was to isolate highly virulent
variants of the virus from sick and dead people, as well as to export
its strains to the USA.
In view of the apparent failure of Metabiota's
activities to meet the goals of controlling the spread of the disease,
the World Health Organisation's Ebola coordinator, Philippe Barbosa,
recommended to recall the staff of the company saying
he was extremely concerned about the potential risks of such
collaboration to WHO's reputation.
The U.S. military contractor's heightened interest
in the Ebola virus is not a coincidence: the disease is one of the most
pathogenic to humans. During the outbreak that began in 2014, 28,000
people were contaminated, over 11,000 of them
died, the mortality rate was around 40%.
The special military operation has led to receiving
documents that reveals the plans of Metabiota and the Ukrainian
Scientific-Technological Centre to study the Ebola virus in Ukraine.
This is the request for U.S. funding to diagnose
highly dangerous pathogens in Ukraine, including Ebola virus. This kind
of requests are part of U.S. strategy to redeploy high-risk work with
dangerous pathogens to third countries.
The research was to be carried out at the Mechnikov
Anti-Plague Institute in Odessa. As the disease is not endemic and has
never been recorded in Ukraine indeed, there is a legitimate question
about the need for such research and its true
purpose.
We have already noted that Ukraine and other
post-Soviet states have become a testing ground for biological weapons
not only for the USA, but also for its NATO allies; on the first place,
Germany. Various projects have been carried out
on behalf of the Joint Medical Service of the German Armed Forces.
Bundeswehr professionals paid particular attention
to the Congo-Crimean fever pathogen. A large-scale screening of the
susceptibility of the local population to this infection was carried out
and included summarising demographic, epidemiological
and clinical data. This kind of approaches allows to identify new
regional virus genotypes and to select strains that cause latent
clinical forms.
The study of natural foci of Crimean-Congo fever
was carried out under the pretext of improving the Ukrainian
epidemiological surveillance system, with the participation of the
Institute of Veterinary Medicine in Kiev and the Mechnikov
Anti-Plague Institute in Odessa.
Bundeswehr's interest in Crimean-Congo fever stems
from the fact that mortality can be as high as 30% and its outbreaks
create a need for lengthy and costly treatment, preventive and special
handling measures.
This is a quote from Bundeswehr's instructions:
'...pay particular attention to fatal cases of infection with
Crimean-Congo fever as it allows the virus strains with maximum
pathogenicity and virulence for humans to be extracted from the
dead individuals...'
Apart from Germany, microbiologists from the USA
have shown a keen interest in tick-borne infections; research in this
area has been funded by DTRA through the UP-1 and UP-8 projects.
A separate project on ixodid ticks that are vectors
of a number of highly dangerous infections (tularemia, West Nile fever,
Congo-Crimean fever) has been implemented by the University of Texas.
Ticks used to be collected in the south-eastern
regions of Ukraine, where natural foci of infections characteristic of
the territory of the Russian Federation are located. At the same time,
the period of implementing this work coincided
with a rapid increase in the incidence of tick-borne borreliosis among
the Ukrainian population, as well as the increase in the number of ticks
in various regions of Russia bordering Ukraine.
This issue is being studied by competent Russian
professionals in coordination with professionals from the Ministry of
Defence of Russia.
We have previously pointed out the significance of
the results of the military-biological projects codenamed UP for the
Pentagon.
Note the report prepared for the U.S. Defence
Department by Black & Veatch and Metabiota. According to the
document, Veterinary Projects codenamed 'TAP' were implemented
simultaneously with the UP projects in Ukraine.
Their main guideline lies in economically
significant quarantine infections capable of damaging the agriculture of
several countries and entire regions, such as glanders, African swine
fever (ASF), classical swine fever, highly pathogenic
avian influenza and Newcastle disease.
African swine fever with two projects dedicated to this pathogen represented particular interest to U.S. military biologists.
The TAP-3 project was aimed to study the spread of
ASF pathogen through wild animals. The migration routes of wild boar
through Ukraine had been examining within its framework. The TAP-6
project scaled this process up to Eastern European
countries.
The study of vector populations of dangerous
zoonotic infections was carried out by staff of the Institute of New
Pathogens of the University of Florida (Gainesville) in Volyn, Rovno,
Zhitomir and Chernigov regions of Ukraine, as well as
in the areas bordering Belarus and Russia.
Note the worsening situation of African swine fever
in Eastern European countries: According to the International Office of
Epizootics, since 2014, outbreaks have been recorded in Latvia (4,021
cases), Estonia (3,814) and Lithuania (4,201).
In Poland, more than 13,000 cases of ASF have been detected, and
agricultural losses from the disease have exceeded 2.4 billion euro.
We have already emphasised the use of biological
weapons in Cuba in the 1970s and 1980s. Today, I would like to focus on
U.S. military-biological activities during the Korean War.
In March 2022, the U.S. Army Strategic Studies
Institute published a report on the U.S. chemical and biological weapons
programme during the Korean War. This report was aimed to create a
possible line of defence against allegations of illegal
activities carried out by U.S. biolaboratories in Ukraine.
The document attempts to refute the testimony of 38
U.S. military pilots who have admitted using biological weapons in
China and Korea.
According to the document, while preparing for the
Korean campaign, '...the U.S. Air Force secured additional funds to
purchase large quantities of chemical and biological munitions, obtained
a testing range for them in Canada and carried
out an extensive conceptual work on their use...'
At that time, the Americans considered brucellosis
pathogens and economically important infections, including wheat stem
rust, as priority biological agents. 2,500 munitions of this type the
U.S. Air Force Strategic Air Command planned
to use, including '...to attack Soviet grain crops...'
Analysis of the data mentioned in the report shows
that the U.S. command uses the results of the research received from the
Japanese military-biological programme and a certain 'continuity' of
the works previously carried out by the Detachment
731 led by Shiro Ishii.
This is the record of the closed session of CIA,
State Department and the Pentagon representatives dated July 7, 1953.
The document clearly shows that the Americans are focusing on techniques
to manipulate public opinion and launch an aggressive
counter-attack within their strategies aimed to defend from
allegations.
The report states that the officials are reluctant
to actual investigations of chemical and biological incidents due to
fears of revealing the activities carried out by the U.S. Eighth Army.
Thus, the comparative analysis of U.S. activities
during the Korean War and currently in Ukraine demonstrates the
persistence of the U.S. policy of building up its own military and
biological capabilities in circumvention of international
agreements.
In conclusion, I would like to present real data on
the health condition of the voluntarily surrendered Ukrainian
servicemen. This diapositive presents the data on presence of antibodies
to contagious disease agents without mentioning personal
data of these servicemen.
The results are as follows: 33% of the examined
servicemen had had hepatitis A, over 4% had renal syndrome fever and 20%
had West Nile fever. The figures are significantly higher than the
statistical average. In view of active research
of these diseases held by the Pentagon within the Ukrainian projects,
there is reason to believe that servicemen of the Armed Forces of
Ukraine (AFU) were involved as volunteers in experiments to assess the
tolerance of dangerous infectious diseases.
The lack of therapeutic effect of antibacterial
medication has been reported during in-patient treatment of AFU
servicemen in medical facilities. High concentrations of antibiotics,
including sulphonyl amides and fluoroquinolones, have
been detected in their blood.
This fact may indicate preventive use of
antibiotics and preparation of personnel for operating in conditions of
biological contamination, such as cholera agent, that indirectly proves
the information of the Russian Defence Ministry that
Ukrainian special units were planning to use biological agents.
The data will be included in the U.S. military-biological dossier and we will continue to examine it and keep you informed.
Existential Dread
-
I'm starting to feel existential angst about how long I have left. More
directly how long active will I be? On the assumption I will become less
active ove...
Gabriel Rockhill, The Pied Piper of Stalinism
-
As interpreted from a Marxist perspective Gabriel Rockhill’s book, Who Paid
the Pipers of Western Marxism? (Monthly Review Press, 2025), is full of
interes...
What Is the Role of Love in the Trump Era?
-
Since the 1980s, blues musician Daryl Davis of Maryland, a black man, has
sought out members of the Ku Klux Klan in an effort to befriend them. His
friends...
Celebrating 113 years of Mama Rosa McCauley Parks
-
*February 4, 1913 -- February 4, 2026*
*Some notes: The life of the courageous activist Mama Rosa McCauley Parks*
Mama Rosa's grandfather Sylvester Ed...
Return of the Magi
-
Lately, the Holy Spirit is in the air. Emotional energy is swirling out of
the earth.I can feel it bubbling up, effervescing and evaporating around
us, s...
Covid-19 Preys Upon The Elderly And The Obese
-
sciencemag | This spring, after days of flulike symptoms and fever, a man
arrived at the emergency room at the University of Vermont Medical Center.
He ...
-
(Damn, has it been THAT long? I don't even know which prompts to use to
post this)
SeeNew
Can't get on your site because you've gone 'invite only'?
Man, ...
First Member of Chumph Cartel Goes to Jail
-
With the profligate racism of the Chumph Cartel, I don’t imagine any of
them convicted and jailed is going to do too much better than your run of
the mill ...