amidwesterndoctor | Much like the vaccine industry, the psychiatric industry will always try to absolve their dangerous medications of responsibility and will aggressively gaslight their victims. Despite these criticisms,there are three facts can be consistently found throughout the literature on akathisia homicides which Gøtzsche argues irrefutably implicate psychiatric medications as the cause of violent homicides:
• These violent events occur in people of all ages, who by all objective and subjective measures were completely normal before the act and where no precipitating factors besides the psychiatric medication could be identified.
• The events were preceded by clear symptoms of akathisia.
• The violent offenders returned to their normal personality when they came off the antidepressant.
Numerous cases where this has happened are summarized within this article from the Palm Beach Post. In most of those cases, a common trend of these spontaneous acts of violence emerges: the act of violence was immediately preceded by a significant change in the psychiatric medications used by the individual. In one case, shortly before committing one of these murders, one of the perpetrators also wrote on a blog that, while taking Prozac, he felt as if he was observing himself "from above."
Individuals with a mutation in the gene that metabolizes psychiatric drugs are much more vulnerable to developing excessive levels of these drugs and triggering severe symptoms such as akathisia and psychosis. There is a good case to be made that individuals with this gene are responsible for many of the horrific acts of iatrogenic (medically induced) violence that occur, however to my knowledge, this is never considered when psychiatric medications are prescribed. Gøtzsche summarized a peer-reviewed forensic investigation of 10 cases where this happened (all but one of these involved an SSRI or an SNRI):
Note: This original version
of this article (which has been revised and updated) was published a
year ago, but sadly is just as pertinent now as it was then. Each time
one of these shootings happen, I watch people get up in arms over what
needs to be done to stop murdering our children, but at the same time
this, the elephant in the room, the clear and irrefutable evidence linking psychiatric medications to homicidal violence is never discussed (which I believe is due their sales making approximately 40 billion dollars a year).
Many
of the stories in here are quite heart wrenching, and I humbly request
that you make the effort to bear witness to these tragic events.
Prior
to the Covid vaccinations, psychiatric medications were the
mass-prescribed medication that had the worst risk-to-benefit ratio on
the market. In addition to rarely providing benefits to patients, there
is a wide range of severe complications that commonly result from
psychiatric medications. Likewise, I and many colleagues believe the
widespread adoption of psychotropic drugs has distorted the cognition of
the demographic of the country which frequently utilizes them (which to
some extent stratifies by political orientation) and has created a wide
range of detrimental shifts in our society.
Selective serotonin reuptake inhibitors (SSRIs) have a similar primary mechanism of action to cocaine. SSRIs block the reuptake of Serotonin, SNRIs, also commonly prescribed block the reuptake of Serotonin and Norepinephrine (henceforth “SSRI refers to both SSRI and SNRI), and Cocaine blocks the reuptake of Serotonin, Norepinephrine, and Dopamine. SSRIs (and SNRIs) were originally used as anti-depressants, then gradually had their use marketed into other areas and along the way have amassed a massive body count.
Once the first SSRI entered the market in 1988, Prozac quickly distinguished itself as a particularly dangerous medication and after nine years, the FDA received 39,000 adverse event reports for Prozac, a number far greater than for any other drug. This included hundreds of suicides, atrocious violent crimes, hostility and aggression, psychosis, confusion, distorted thinking, convulsions, amnesia, and sexual dysfunction (long-term or permanent sexual dysfunction is one of the most commonly reported side effects from anti-depressants, which is ironic given that the medication is supposed to make you less, not more depressed).
SSRI homicides are common, and a website exists that has compiled thousands upon thousands of documented occurrences. As far as I know (there are most likely a few exceptions), in all cases where a mass school shooting has happened, and it was possible to know the medical history of the shooter, the shooter was taking a psychiatric medication that was known for causing these behavioral changes. After each mass shooting, memes illustrating this topic typically circulate online, and the recent events in Texas [this article was written shortly after the shooting last year] are no exception. I found one of these and made an updates version of it (the one I originally used contained some inaccuracies)
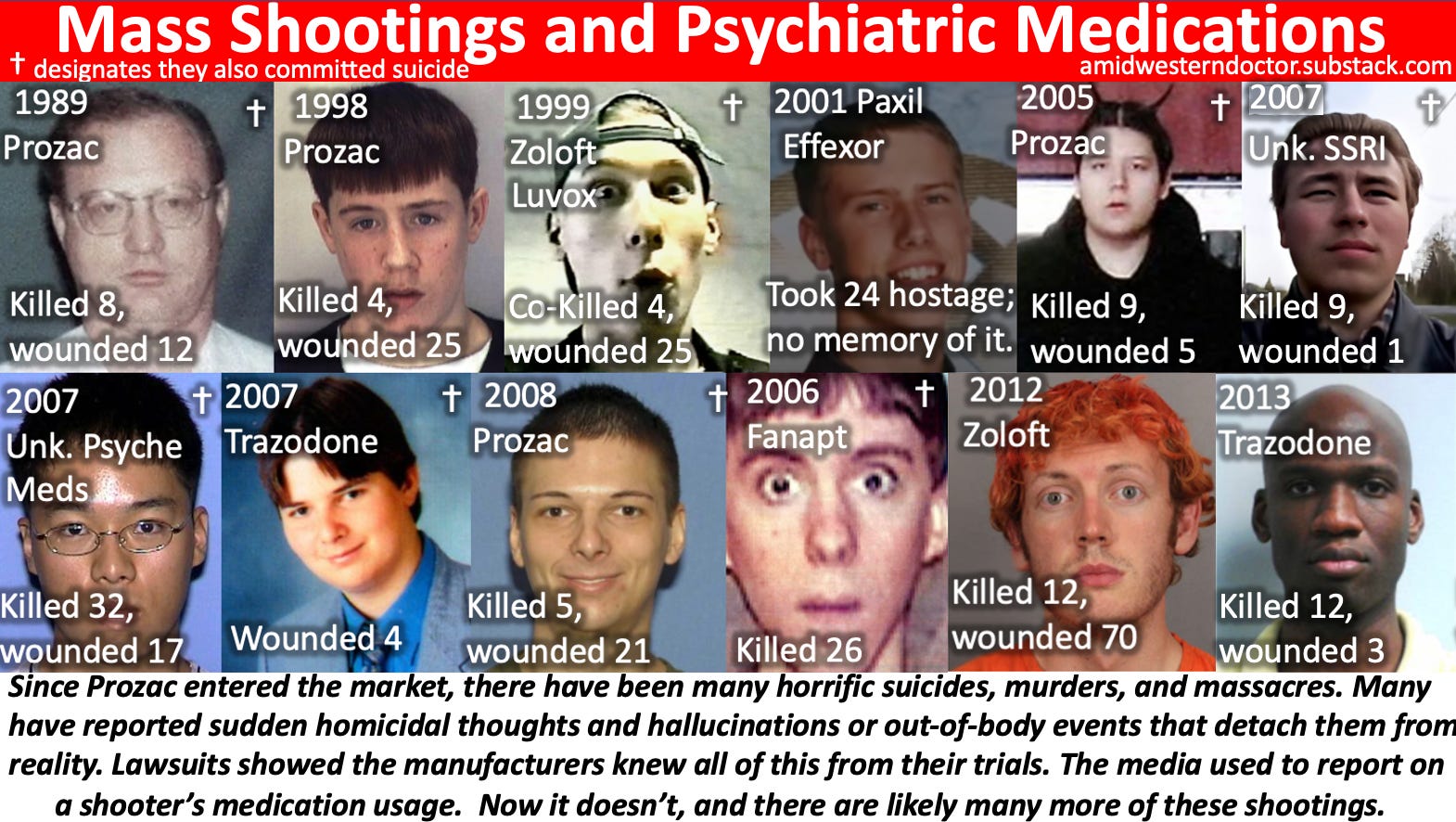
Oftentimes, “SSRIs cause mass shootings” is treated as just another crazy conspiracy theory. However, much in the same way the claim “COVID Vaccines are NOT safe and effective” is typically written off as a conspiracy theory, if you go past these labels and dig into the actual data, an abundantly clear and highly concerning picture emerges.
There are many serious issues with psychiatric medications. For brevity, this article will exclusively focus on their tendency to cause horrific violent crimes. This was known long before they entered the market by both the drug companies and the FDA. While there is a large amount of evidence for this correlation, it is the one topic that is never up for debate when a mass shooting occurs. I have a lot of flexibility to discuss highly controversial topics with my colleagues, but this topic is met with so much hostility that I can never bring it up. It is, for this reason, I am immensely grateful to have an anonymous forum I can use.



