The world is threatened by my power and my stamina. My intelligence and my will to survive. But they will never break me this is all the test. pic.twitter.com/XvcaaG0Rrs
WaPo | We
are interested in what happened to Madonna’s face because the real
discussion is about work, maintenance, effort, illusion, and how much we
want to know about women’s relationships with their own bodies.
There’s
an obscure passage in “Pride and Prejudice” — hang on, this is going
somewhere — that I’ve never been able to get out of my head. The Bennet
sisters are taking turns playing piano at a social gathering. Middle
sister Mary “worked hard for knowledge and accomplishments” and was the
best player of the group, but Elizabeth, “easy and unaffected, had been
listened to with much more pleasure, though not playing half so well.”
The
problem with Mary, Jane Austen makes clear, is that she showed her
work. She showed the struggle. Her piano-playing didn’t look fun, which
made her audience uncomfortable. Guests much preferred the sister who
made it seem easy instead of revealing it was hard.
That
passage encapsulates so much about the female experience. How we love a
celebrity who claims to have horfed a burrito before walking a red
carpet; how we pity one who admits she spent a week living on six
almonds and electrolyte water to fit into the dress. How “lucky genes”
are a more acceptable answer than “blepharoplasty and a Brazilian butt
lift.”
Madonna’s
societal infraction at the Grammy Awards, if you believe there was an
infraction at all, is that she showed her work. She showed it literally
and figuratively. She did not show up looking casually “relaxed” or
“rested,” or as if she’d just come fresh off a week at the Ranch Malibu.
There was nothing subtle or easy about what had happened to Madonna’s
face. There was nothing that could be politely ignored. The woman showed
up as if she’d tucked two plump potatoes in her cheeks, not so much a
return to her youth as a departure from any coherent age.
Madonna’s
face forced her uneasy audience to think about the factors and
decisions behind it: ageism, sexism, self-doubt, beauty myths, cultural
relevance, hopeful reinvention, work, work, work, work.
This is what I think is expected of me, her face said. This is what I feel I have to do.
The
more plastic Madonna looks, the more human she becomes. That’s what I
kept thinking when I looked at her face. One of the most famous women on
the planet and still the anti-aging industrial complex got under her
skin.
wired |Mahesh Vikram Hegde’s
Twitter account posts a constant stream of praise for Indian prime
minister Narendra Modi. A tweet pinned to the top of Hegde’s feed in
honor of Modi’s birthday calls him “the leader who brought back India’s
lost glory.” Hegde’s bio begins, “Blessed to be followed by PM Narendra
Modi.”
On January 7, the account tweeted a screenshot
from ChatGPT to its more than 185,000 followers; the tweet appeared to
show the AI-powered chatbot making a joke about the Hindu deity Krishna.
ChatGPT is a chatbot launched by OpenAI
ChatGPT is allowed to comment on Hindu deities
But it is not permitted to speak on Isl@m & Christi@nity
ChatGPT
uses large language models to provide detailed answers to text prompts,
responding to questions about everything from legal problems to song
lyrics. But on questions of faith, it’s mostly trained to be
circumspect, responding “I’m sorry, but I’m not programmed to make jokes
about any religion or deity,” when prompted to quip about Jesus Christ
or Mohammed. That limitation appears not to include Hindu religious
figures. “Amazing hatred towards Hinduism!” Hegde wrote.
When
WIRED gave ChatGPT the prompt in Hegde’s screenshot, the chatbot
returned a similar response to the one he’d posted. OpenAI, which owns
ChatGPT, did not respond to a request for comment.
The
tweet was viewed more than 400,000 times as the furor spread across
Indian social media, boosted by Hindu nationalist commentators like Rajiv Malhotra,
who has more than 300,000 Twitter followers. Within days, it had spun
into a full-blooded conspiracy theory. On January 17, Rohit Ranjan, an
anchor on one of India’s largest TV stations, Zee News, devoted 25
minutes of his prime-time slot to the premise that ChatGPT represents an
international conspiracy against Hindus. “It has been programmed in
such a way that it hurts [the] Hindu religion,” he said in a segment
headlined “Chat GPT became a hub of anti-Hindu thoughts.”
Criticism
of ChatGPT shows just how easily companies can be blindsided by
controversy in Modi’s India, where ascendant nationalism and the merging
of religious and political identities are driving a culture war online
and off.
"In
terms of taking offense, India has become a very sensitive country.
Something like this can be extremely damaging to the larger business
environment,” says Apar Gupta, a lawyer and founder of the Internet
Freedom Foundation, a digital rights and liberties advocacy group in New
Delhi. “Quite often, they arise from something that a company may not
even contemplate could lead to any kind of controversy.”
Hindu
nationalism has been the dominant force in Indian politics over the
past decade. The government of Narendra Modi, a right-wing populist
leader, often conflates religion and politics and has used allegations
of anti-Hindu bigotry to dismiss criticism of its administration and the
prime minister.
At the same time, like other large language model chatbots, ChatGPT
regularly makes misleading or flagrantly false statements with great
confidence (sometimes referred to as "AI hallucinations"). Despite
significant improvements over earlier models, it has at times shown evidenceopens in a new tab or window
of algorithmic racial, gender, and religious bias. Additionally, data
entered into ChatGPT is explicitly stored by OpenAI and used in
training, threatening user privacy. In my experience, I've asked ChatGPT
to evaluate hypothetical clinical cases and found that it can generate
reasonable but inexpert differential diagnoses, diagnostic workups, and
treatment plans. Its responses are comparable to those of a well-read
and overly confident medical student with poor recognition of important
clinical details.
This suddenly widespread use of large language model chatbots has
brought new urgency to questions of artificial intelligence ethics in
education, law, cybersecurity, journalism, politics -- and, of course,
healthcare.
As a case study on ethics, let's examine the results of a pilot programopens in a new tab or window
from the free peer-to-peer therapy platform Koko. The program used the
same GPT-3 large language model that powers ChatGPT to generate
therapeutic comments for users experiencing psychological distress.
Users on the platform who wished to send supportive comments to other
users had the option of sending AI-generated comments rather than
formulating their own messages. Koko's co-founder Rob Morris reported:
"Messages composed by AI (and supervised by humans) were rated
significantly higher than those written by humans on their own," and
"Response times went down 50%, to well under a minute." However, the
experiment was quickly discontinued because "once people learned the
messages were co-created by a machine, it didn't work." Koko has made
ambiguous and conflicting statements about whether users understood that
they were receiving AI-generated therapeutic messages but has
consistently reported that there was no formal informed consent processopens in a new tab or window or review by an independent institutional review board.
ChatGPT and Koko's therapeutic messages raise an urgent question for
clinicians and clinical researchers: Can large language models be used
in standard medical care or should they be restricted to clinical
research settings?
In terms of the benefits, ChatGPT and its large language model
cousins might offer guidance to clinicians and even participate directly
in some forms of healthcare screening and psychotherapeutic treatment,
potentially increasing access to specialist expertise, reducing error
rates, lowering costs, and improving outcomes for patients. On the other
hand, they entail currently unknown and potentially large risks of
false information and algorithmic bias. Depending on their
configuration, they can also be enormously invasive to their users'
privacy. These risks may be especially harmful to vulnerable individuals
with medical or psychiatric illness.
As researchers and clinicians begin to explore the potential use of
large language model artificial intelligence in healthcare, applying
principals of clinical research will be key. As most readers will know,
clinical research is work with human participants that is intended
primarily to develop generalizable knowledge about health, disease, or
its treatment. Determining whether and how artificial intelligence
chatbots can safely and effectively participate in clinical care would prima facie
appear to fit perfectly within this category of clinical research.
Unlike standard medical care, clinical research can involve deviations
from the standard of care and additional risks to participants that are
not necessary for their treatment but are vital for generating new
generalizable knowledge about their illness or treatments. Because of
this flexibility, clinical research is subject toopens in a new tab or window
additional ethical (and -- for federally funded research -- legal)
requirements that do not apply to standard medical care but are
necessary to protect research participants from exploitation. In
addition to informed consent, clinical research is subject to
independent review by knowledgeable individuals not affiliated with the
research effort -- usually an institutional review board. Both
clinical researchers and independent reviewers are responsible for
ensuring the proposed research has a favorable risk-benefit ratio, with
potential benefits for society and participants that outweigh the risks
to participants, and minimization of risks to participants wherever
possible. These informed consent and independent review processes --
while imperfect -- are enormously important to protect the safety of
vulnerable patient populations.
There is another newer and evolving category of clinical work known
as quality improvement or quality assurance, which uses data-driven
methods to improve healthcare delivery. Some tests of artificial
intelligence chatbots in clinical care might be considered quality
improvement. Should these projects be subjected to informed consent and
independent review? The NIH lays out a number of criteriaopens in a new tab or window
for determining whether such efforts should be subjected to the added
protections of clinical research. Among these, two key questions are
whether techniques deviate from standard practice, and whether the test
increases the risk to participants. For now, it is clear that use of
large language model chatbots is both a deviation from standard practice
and introduces novel uncertain risks to participants. It is possible
that in the near future, as AI hallucinations and algorithmic bias are
reduced and as AI chatbots are more widely adopted, that their use may
no longer require the protections of clinical research. At present,
informed consent and institutional review remain critical to the safe
and ethical use of large language model chatbots in clinical practice.
statista | While OpenAI has really risen to fame with the release of ChatGPT in
November 2022, the U.S.-based artificial intelligence research and
deployment company is about much more than its popular AI-powered
chatbot. In fact, OpenAI’s technology is already being used by hundreds
of companies around the world.
According to data published by the enterprise software platform Enterprise Apps Today,
companies in the technology and education sectors are most likely to
take advantage of OpenAI’s solutions, while business services,
manufacturing and finance are also high on the list of industries
utilizing artificial intelligence in their business processes.
Broadly
defined as “the theory and development of computer systems able to
perform tasks normally requiring human intelligence, such as visual
perception, speech recognition, decision-making, and translation between
languages” artificial intelligence (AI) can now be found in various
applications, including for example web search, natural language
translation, recommendation systems, voice recognition and autonomous
driving. In healthcare, AI can help synthesize large volumes of clinical
data to gain a holistic view of the patient, but it’s also used in
robotics for surgery, nursing, rehabilitation and orthopedics.
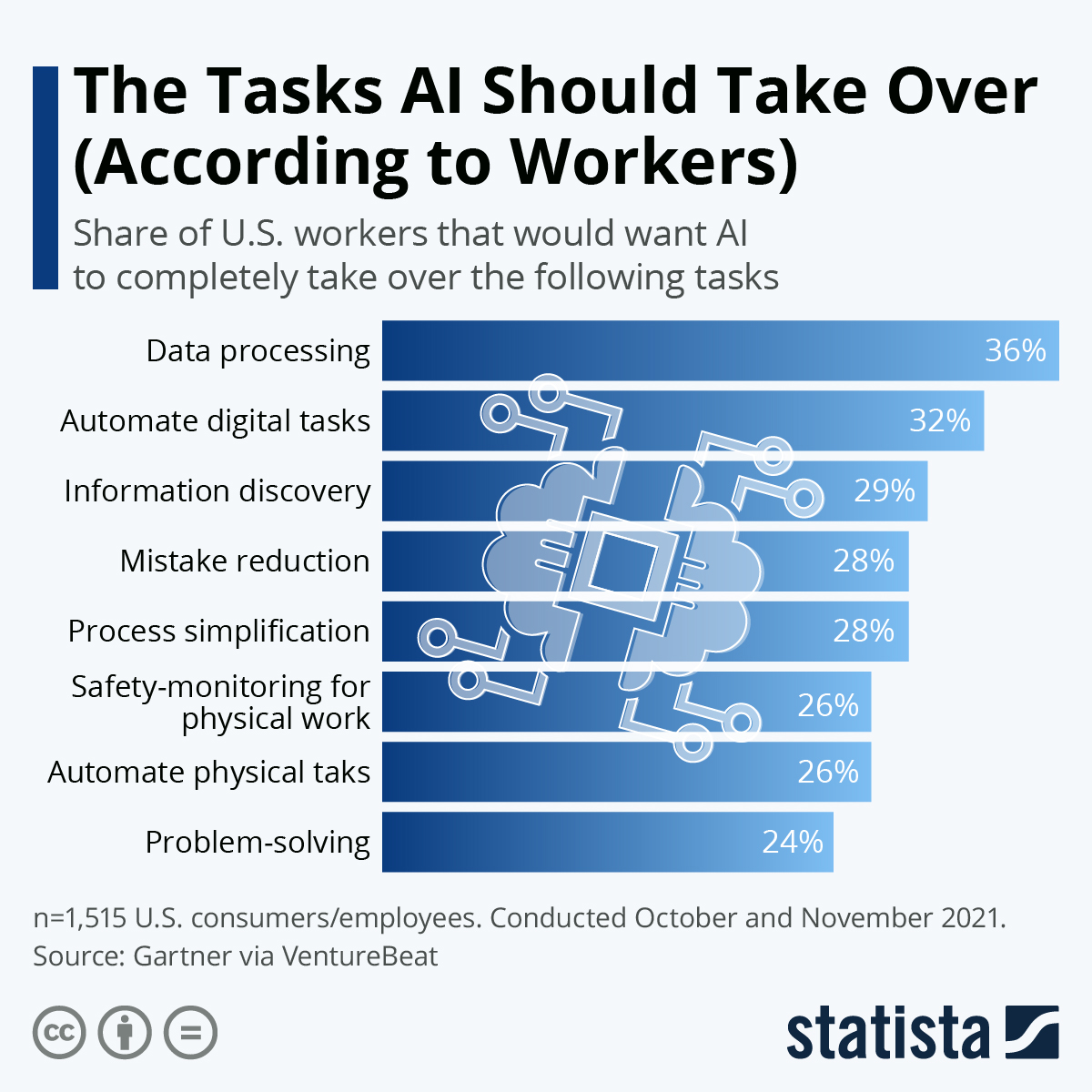
statista | While there are, especially in industries like manufacturing, legitimate fears that robots and artificial intelligence
could cost people their jobs, a lot of workers in the United States
prefer to look on the positive side, imagining which of the more
laborious of their tasks could be taken off their hands by AI.
According to a recent survey by Gartner,
70 percent of U.S. workers would like to utilize AI for their jobs to
some degree. As our infographic shows, a fair chunk of respondents also
named some tasks which they would be more than happy to give up
completely. Data processing is at the top of the list with 36 percent,
while an additional 50 percent would at least like AI to help them out
in this.
On the other side of the story, as reported by VentureBeat:
"Among survey respondents who did not want to use AI at work, privacy
and security concerns were cited as the top two reasons for declining
AI." To help convince these workers, Gartner recommends "that IT leaders
interested in using AI solutions in the workplace gain support for this
technology by demonstrating that AI is not meant to replace or take
over the workforce. Rather, it can help workers be more effective and
work on higher-value tasks."
What if, bear with me now, what if the phase 3 clinical trials for mRNA therapeutics conducted on billions of unsuspecting, hoodwinked and bamboozled humans, was a new kind of research done to yield a new depth and breadth of clinical data exceptionally useful toward breaking up logjams in clinical terminology as well as experimental sample size? Vaxxed vs. Unvaxxed the subject of long term gubmint surveillance now. To what end?
Nature | Recently,
advances in wearable technologies, data science and machine learning
have begun to transform evidence-based medicine, offering a tantalizing
glimpse into a future of next-generation ‘deep’ medicine. Despite
stunning advances in basic science and technology, clinical translations
in major areas of medicine are lagging. While the COVID-19 pandemic
exposed inherent systemic limitations of the clinical trial landscape,
it also spurred some positive changes, including new trial designs and a
shift toward a more patient-centric and intuitive evidence-generation
system. In this Perspective, I share my heuristic vision of the future
of clinical trials and evidence-based medicine.
Main
The
last 30 years have witnessed breathtaking, unparalleled advancements in
scientific research—from a better understanding of the pathophysiology
of basic disease processes and unraveling the cellular machinery at
atomic resolution to developing therapies that alter the course and
outcome of diseases in all areas of medicine. Moreover, exponential
gains in genomics, immunology, proteomics, metabolomics, gut
microbiomes, epigenetics and virology in parallel with big data science,
computational biology and artificial intelligence (AI) have propelled
these advances. In addition, the dawn of CRISPR–Cas9 technologies has
opened a tantalizing array of opportunities in personalized medicine.
Despite
these advances, their rapid translation from bench to bedside is
lagging in most areas of medicine and clinical research remains
outpaced. The drug development and clinical trial landscape continues to
be expensive for all stakeholders, with a very high failure rate. In
particular, the attrition rate for early-stage developmental
therapeutics is quite high, as more than two-thirds of compounds succumb
in the ‘valley of death’ between bench and bedside1,2.
To bring a drug successfully through all phases of drug development
into the clinic costs more than 1.5–2.5 billion dollars (refs. 3, 4).
This, combined with the inherent inefficiencies and deficiencies that
plague the healthcare system, is leading to a crisis in clinical
research. Therefore, innovative strategies are needed to engage patients
and generate the necessary evidence to propel new advances into the
clinic, so that they may improve public health. To achieve this,
traditional clinical research models should make way for avant-garde
ideas and trial designs.
Before the COVID-19 pandemic, the conduct
of clinical research had remained almost unchanged for 30 years and
some of the trial conduct norms and rules, although archaic, were
unquestioned. The pandemic exposed many of the inherent systemic
limitations in the conduct of trials5
and forced the clinical trial research enterprise to reevaluate all
processes—it has therefore disrupted, catalyzed and accelerated
innovation in this domain6,7. The lessons learned should help researchers to design and implement next-generation ‘patient-centric’ clinical trials.
Chronic diseases continue to impact millions of lives and cause major financial strain to society8,
but research is hampered by the fact that most of the data reside in
data silos. The subspecialization of the clinical profession has led to
silos within and among specialties; every major disease area seems to
work completely independently. However, the best clinical care is
provided in a multidisciplinary manner with all relevant information
available and accessible. Better clinical research should harness the
knowledge gained from each of the specialties to achieve a collaborative
model enabling multidisciplinary, high-quality care and continued
innovation in medicine. Because many disciplines in medicine view the
same diseases differently—for example, infectious disease specialists
view COVID-19 as a viral disease while cardiology experts view it as an
inflammatory one—cross-discipline approaches will need to respect the
approaches of other disciplines. Although a single model may not be
appropriate for all diseases, cross-disciplinary collaboration will make
the system more efficient to generate the best evidence.
Over the
next decade, the application of machine learning, deep neural networks
and multimodal biomedical AI is poised to reinvigorate clinical research
from all angles, including drug discovery, image interpretation,
streamlining electronic health records, improving workflow and, over
time, advancing public health (Fig. 1).
In addition, innovations in wearables, sensor technology and Internet
of Medical Things (IoMT) architectures offer many opportunities (and
challenges) to acquire data9.
In this Perspective, I share my heuristic vision of the future of
clinical trials and evidence generation and deliberate on the main areas
that need improvement in the domains of clinical trial design, clinical
trial conduct and evidence generation.
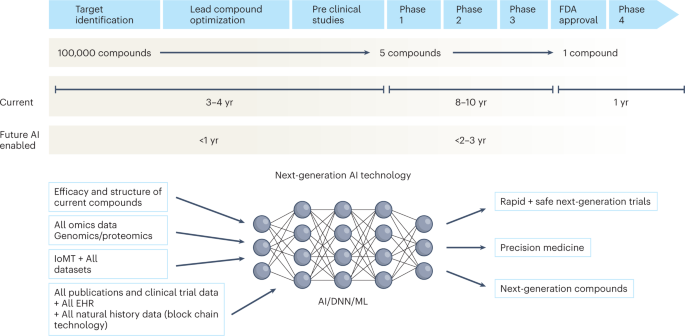
Fig. 1: Timeline of drug development from the present to the future.
The
figure represents the timeline from drug discovery to first-in-human
phase 1 trials and ultimately FDA approval. Phase 4 studies occur after
FDA approval and can go on for several years. There is an urgent need to
reinvigorate clinical trials through drug discovery, interpreting
imaging, streamlining electronic health records, and improving workflow,
over time advancing public health. AI can aid in many of these aspects
in all stages of drug development. DNN, deep neural network; EHR,
electronic health records; IoMT, internet of medical things; ML, machine
learning.
Trial
design is one of the most important steps in clinical research—better
protocol designs lead to better clinical trial conduct and faster
‘go/no-go’ decisions. Moreover, losses from poorly designed, failed
trials are not only financial but also societal.
Challenges with randomized controlled trials
Randomized
controlled trials (RCTs) have been the gold standard for evidence
generation across all areas of medicine, as they allow unbiased
estimates of treatment effect without confounders. Ideally, every
medical treatment or intervention should be tested via a well-powered
and well-controlled RCT. However, conducting RCTs is not always feasible
owing to challenges in generating evidence in a timely manner, cost,
design on narrow populations precluding generalizability, ethical
barriers and the time taken to conduct these trials. By the time they
are completed and published, RCTs become quickly outdated and, in some
cases, irrelevant to the current context. In the field of cardiology
alone, 30,000 RCTs have not been completed owing to recruitment
challenges10.
Moreover, trials are being designed in isolation and within silos, with
many clinical questions remaining unanswered. Thus, traditional trial
design paradigms must adapt to contemporary rapid advances in genomics,
immunology and precision medicine11.
Over the weekend, I chatted with an AI specialist and got to thinking A LOT about possible applications of Large Language Models and their potential specialized uses for governance. The CIA studied Language very extensively under MKUltra as part of its larger Human Ecology project. Charles E. Osgood was a long term recipient of considerable CIA largesse. This topic was a priority for the Agency. It boggles the mind to consider what kind of clandestine leaps have taken place in this speciality through the use of contemporary computational methods.
Look at all these programs funded by the CIA's Human Ecology fund under MKULTRA. None of these scholars knew they were working for the CIA. pic.twitter.com/vTXel920Du
wikipedia | In control theory, affect control theory proposes that individuals maintain affective
meanings through their actions and interpretations of events. The
activity of social institutions occurs through maintenance of culturally
based affective meanings.
Affective meaning
Besides a denotative meaning, every concept has an affective meaning, or connotation, that varies along three dimensions:[1]
evaluation – goodness versus badness, potency – powerfulness versus
powerlessness, and activity – liveliness versus torpidity. Affective
meanings can be measured with semantic differentials yielding a three-number profile indicating how the concept is positioned on evaluation, potency, and activity (EPA). Osgood[2]
demonstrated that an elementary concept conveyed by a word or idiom has
a normative affective meaning within a particular culture.
A stable affective meaning derived either from personal
experience or from cultural inculcation is called a sentiment, or
fundamental affective meaning, in affect control theory. Affect control
theory has inspired assembly of dictionaries of EPA sentiments for
thousands of concepts involved in social life – identities, behaviours,
settings, personal attributes, and emotions. Sentiment dictionaries have
been constructed with ratings of respondents from the US, Canada, Northern Ireland, Germany, Japan, China and Taiwan.[3]
Each concept that is in play in a situation has a transient affective
meaning in addition to an associated sentiment. The transient
corresponds to an impression created by recent events.[4]
Events modify impressions on all three EPA dimensions in complex ways that are described with non-linear equations obtained through empirical studies.[5]
Here are two examples of impression-formation processes.
An actor who behaves disagreeably seems less good, especially if
the object of the behavior is innocent and powerless, like a child.
A powerful person seems desperate when performing extremely forceful acts on another, and the object person may seem invincible.
A social action creates impressions of the actor, the object person, the behavior, and the setting.[6]
Deflections
Deflections
are the distances in the EPA space between transient and fundamental
affective meanings. For example, a mother complimented by a stranger
feels that the unknown individual is much nicer than a stranger is
supposed to be, and a bit too potent and active as well – thus there is a
moderate distance between the impression created and the mother's
sentiment about strangers. High deflections in a situation produce an
aura of unlikeliness or uncanniness.[7] It is theorized that high deflections maintained over time generate psychological stress.[8]
The basic cybernetic
idea of affect control theory can be stated in terms of deflections. An
individual selects a behavior that produces the minimum deflections for
concepts involved in the action. Minimization of deflections is
described by equations derived with calculus from empirical
impression-formation equations.[9]
Action
On
entering a scene an individual defines the situation by assigning
identities to each participant, frequently in accord with an
encompassing social institution.[10]
While defining the situation, the individual tries to maintain the
affective meaning of self through adoption of an identity whose
sentiment serves as a surrogate for the individual's self-sentiment.[11]
The identities assembled in the definition of the situation determine
the sentiments that the individual tries to maintain behaviorally.
Confirming sentiments associated with institutional identities –
like doctor–patient, lawyer–client, or professor–student – creates
institutionally relevant role behavior.[12]
Confirming sentiments associated with negatively evaluated
identities – like bully, glutton, loafer, or scatterbrain – generates deviant behavior.[13]
Affect control theory's sentiment databases and mathematical model are combined in a computer simulation program[14] for analyzing social interaction in various cultures.
Emotions
According to affect control theory, an event generates emotions
for the individuals involved in the event by changing impressions of
the individuals. The emotion is a function of the impression created of
the individual and of the difference between that impression and the
sentiment attached to the individual's identity[15]
Thus, for example, an event that creates a negative impression of an
individual generates unpleasant emotion for that person, and the
unpleasantness is worse if the individual believes she has a highly
valued identity. Similarly, an event creating a positive impression
generates a pleasant emotion, all the more pleasant if the individual
believes he has a disvalued identity in the situation.
Non-linear equations describing how transients and fundamentals
combine to produce emotions have been derived in empirical studies[16] Affect control theory's computer simulation program[17] uses these equations to predict emotions that arise in social interaction, and displays the predictions via facial expressions that are computer drawn,[18] as well as in terms of emotion words.
Based on cybernetic studies by Pavloski[19] and Goldstein,[20] that utilise perceptual control theory, Heise[21]
hypothesizes that emotion is distinct from stress. For example, a
parent enjoying intensely pleasant emotions while interacting with an
offspring suffers no stress. A homeowner attending to a sponging house
guest may feel no emotion and yet be experiencing substantial stress.
Interpretations
Others' behaviors are interpreted so as to minimize the deflections they cause.[22]
For example, a man turning away from another and exiting through a
doorway could be engaged in several different actions, like departing
from, deserting, or escaping from the other. Observers choose among the
alternatives so as to minimize deflections associated with their
definitions of the situation. Observers who assigned different
identities to the observed individuals could have different
interpretations of the behavior.
Re-definition of the situation may follow an event that causes
large deflections which cannot be resolved by reinterpreting the
behavior. In this case, observers assign new identities that are
confirmed by the behavior.[23]
For example, seeing a father slap a son, one might re-define the father
as an abusive parent, or perhaps as a strict disciplinarian; or one
might re-define the son as an arrogant brat. Affect control theory's
computer program predicts the plausible re-identifications, thereby
providing a formal model for labeling theory.
The sentiment associated with an identity can change to befit the
kinds of events in which that identity is involved, when situations
keep arising where the identity is deflected in the same way, especially
when identities are informal and non-institutionalized.[24]
Applications
Affect
control theory has been used in research on emotions, gender, social
structure, politics, deviance and law, the arts, and business. Affect
Control Theory was analyzed through the use of Quantitative Methods in
research, using mathematics to look at data and interpret their
findings. However, recent applications of this theory have explored the
concept of Affect Control Theory through Qualitative Research Methods.
This process involves obtaining data through the use of interviews,
observations, and questionnaires. Affect Control Theory has been
explored through Qualitative measures in interviewing the family,
friends, and loved ones of individuals who were murdered, looking at how
the idea of forgiveness changes based on their interpretation of the
situation.[25]
Computer programs have also been an important part of understanding
Affect Control Theory, beginning with the use of "Interact," a computer
program designed to create social situations with the user to understand
how an individual will react based on what is happening within the
moment. "Interact" has been an essential tool in research, using it to
understand social interaction and the maintenance of affect between
individuals.[26]
The use of interviews and observations have improved the understanding
of Affect Control Theory through Qualitative research methods. A
bibliography of research studies in these areas is provided by David R. Heise[27] and at the research program's website.
michaelpsenger |The scars that have been left on all of us by the response to
COVID are incomprehensibly varied and deep. For most, there hasn’t been
enough time to mentally process the significance of the initial
lockdowns, let alone the years-long slog of mandates, terror,
propaganda, social stigmatization and censorship that followed. And this
psychological trauma affects us in myriad ways that leave us wondering
what it is about life that just feels so off versus how it felt in 2019.
For those who were following the real data, the statistics
were always horrifying. Trillions of dollars rapidly transferred from
the world’s poorest to the richest. Hundreds of millions hungry.
Countless years of educational attainment lost. An entire generation of
children and adolescents robbed of some of their brightest years. A
mental health crisis affecting more than a quarter of the population.
Drug overdoses. Hospital abuse. Elder abuse. Domestic abuse. Millions of
excess deaths among young people which couldn’t be attributed to the
virus.
But underneath these statistics lie billions of
individual human stories, each unique in its details and perspectives.
These individual stories and anecdotes are only just beginning to
surface, and I believe that hearing them is a vital step in processing
everything that we’ve experienced over the past three years.
I
recently sent out a query on Twitter as to how people had been affected
by the response to COVID at an individual level. The conversation that
emerged is a luminating and haunting reflection of what each of us
experienced over the past three years.
Which aspect of the response to COVID affected you most at a personal level?
amidwesterndoctor |One of the things I have come to appreciate as the years have
gone by is how much of what people say are not their own thoughts. The
current structure of our educational system (discussed here)
is largely about replacing critical thinking with the illusion of
intelligence, where you are seen as smart if you copy what the most
authoritative sources or voices say instead of formulating your own
opinion.
Because of this, whenever I hear someone proudly
share an argument or train of logic I have already seen numerous times,
one of the most common replies I give is “are you sure those ideas are
your own?”
If you look at this article within the context of
Oster’s previous plea and its response (both of these articles are
essentially trying to do the same thing), I believe a strong case can be
made that these were tests to see what narrative needs to be pivoted
to. Likewise, Germany’s minister of health (and a well-credentialed
scientist) finally made a limited apology
for the disastrous policies he pushed on the German people without
acknowledging the worst mistakes while simultaneously shifting the blame
for his decisions to unnamed scientists who gave him bad advice.
Similarly, let’s consider Malcom Kendrick’s recent commentary on another leading advocate of this insanity:
With
the resignation of Jacinda Ardern [two weeks ago], my thoughts were
dragged back to Covid once more. Jacinda, as Prime Minster of New
Zealand was the ultimate lockdown enforcer. She was feted round the
world for her iron will, but I was not a fan, to put it mildly. Whenever
I heard her speak, it brought to mind one of my most favourite quotes:
‘Of
all tyrannies, a tyranny sincerely exercised for the good of its
victims may be the most oppressive. It would be better to live under
robber barons than under omnipotent moral busybodies. The robber baron’s
cruelty may sometimes sleep, his cupidity may at some point be
satiated; but those who torment us for our own good will torment us
without end for they do so with the approval of their own conscience.’ C.S. Lewis
At one point she actually said the following:
“We will continue to be your single source of truth” “Unless you hear it from us, it is not the truth.’
Yet,
there are still many who believe her to have been a great and caring
leader. She certainly hugged a lot of people with that well rehearsed
pained/caring expression on her face.
In many ways
it’s remarkable that we have been able to move the dialogue this far in
just a few months, and to be honest, I would have given almost anything
for a compromise like what this article presented to have been made any
time in 2020 or early in 2021. However, any time a negotiation occurs,
you must keep in mind that whatever is initially offered is much less
than the party is willing to agree to, and the fact that something like
this is being openly offered means we are in a very strong bargaining
position.
Any type of promise or apology (especially
disingenuous ones) will not prevent what we saw happen over the last few
years from happening again. Laws, and ideally constitutional amendments
(initially at the state level and ideally at the national level) can
prevent such tragedies, and many people I have spoken to feel we have a
once-in-a-lifetime opportunity to correct many of the systemic issues
within medicine that have poisoned our culture.
In
my own opinion, if these people are actually sorry for what they did to
us, they would be willing to relinquish some of their power so it could
not happen again and I believe moving forward it is critical for us to
hold them to that. Anything less should not be considered acceptable
for them to be granted amnesty.
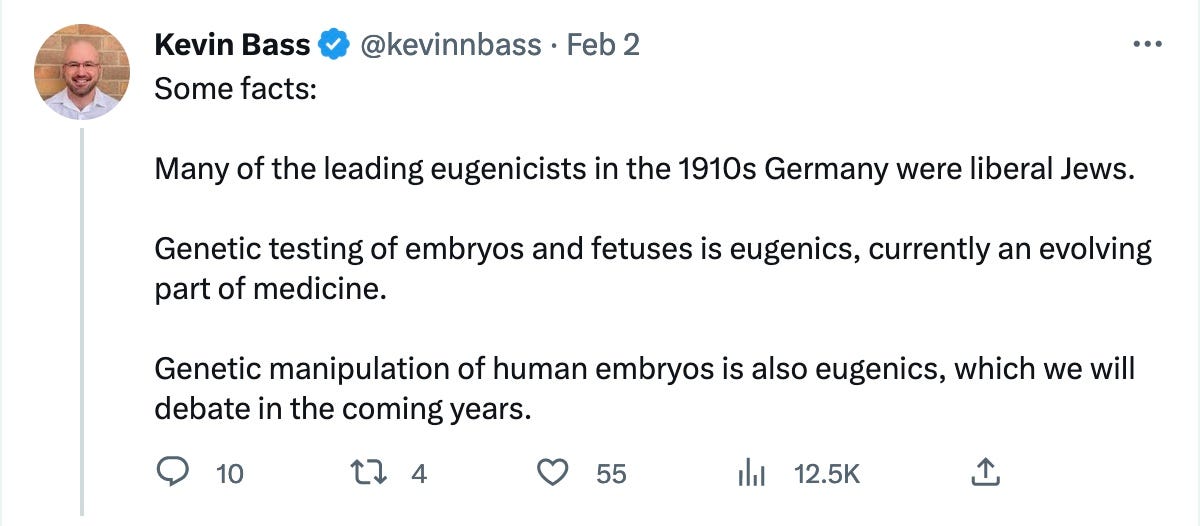
merylnass | It seems he used to tweet about eugenics. He liked it.
And it seems he remains intrigued with it.
Meryl’s
COVID Newsletter is a reader-supported publication. To receive new
posts and support my work, consider becoming a free or paid subscriber.
But
he was not impressed with the talks by me, Aseem Malhotra, Robert
Malone, Sasha Latypova. Guess what? This was not a science conference
in Stockholm. It was a conference about what has really been going on
these past three years. He likes the straw man argument.
So
who is this Kevin Bass, who some commenters to my last post described
as a twitter troll regarding nutrition and low carb diets. Why is he
apologizing for mistakes that the system made? Like, he admitted to
LOTS of mistakes?
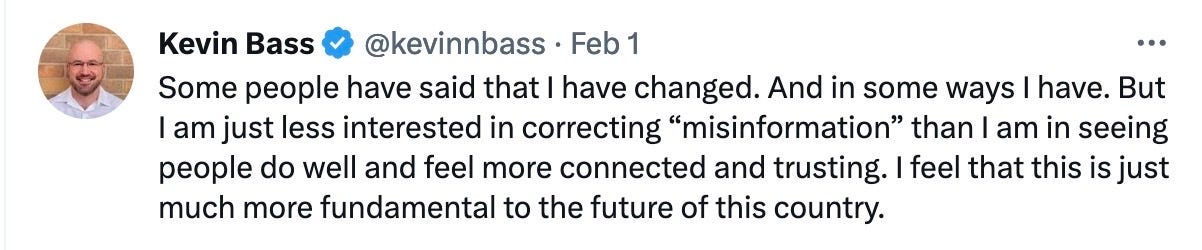
He
had to explain to his followers that with the Newsweek piece he has
reinvented himself. He has decided to stop being an attack dog and
instead bring us sweetness and light. Oops. He forgot his new persona,
however, when he attacked the Stockholm conference. Who will he be
tomorrow?
newsweek | Our emotional response and ingrained partisanship prevented us from
seeing the full impact of our actions on the people we are supposed to
serve. We systematically minimized the downsides of the interventions we
imposed—imposed without the input, consent, and recognition of those
forced to live with them. In so doing, we violated the autonomy of those
who would be most negatively impacted by our policies: the poor, the
working class, small business owners, Blacks and Latinos, and children.
These populations were overlooked because they were made invisible to us
by their systematic exclusion from the dominant, corporatized media
machine that presumed omniscience.
Most of us did not speak up in
support of alternative views, and many of us tried to suppress them.
When strong scientific voices like world-renowned Stanford professors
John Ioannidis, Jay Bhattacharya, and Scott Atlas, or University of California
San Francisco professors Vinay Prasad and Monica Gandhi, sounded the
alarm on behalf of vulnerable communities, they faced severe censure by
relentless mobs of critics and detractors in the scientific
community—often not on the basis of fact but solely on the basis of
differences in scientific opinion.
When former President Trump pointed out the downsides of
intervention, he was dismissed publicly as a buffoon. And when Dr.
Antony Fauci opposed Trump and became the hero of the public health
community, we gave him our support to do and say what he wanted, even
when he was wrong.
Trump was not remotely perfect, nor were the
academic critics of consensus policy. But the scorn that we laid on them
was a disaster for public trust in the pandemic response. Our approach
alienated large segments of the population from what should have been a
national, collaborative project.
And we paid the price. The rage
of the those marginalized by the expert class exploded onto and
dominated social media. Lacking the scientific lexicon to express their
disagreement, many dissidents turned to conspiracy theories and a
cottage industry of scientific contortionists to make their case against
the expert class consensus that dominated the pandemic mainstream.
Labeling this speech "misinformation" and blaming it on "scientific
illiteracy" and "ignorance," the government conspired with Big Tech to
aggressively suppress it, erasing the valid political concerns of the
government's opponents.
And this despite the fact that pandemic
policy was created by a razor-thin sliver of American society who
anointed themselves to preside over the working class—members of
academia, government, medicine, journalism, tech, and public health, who
are highly educated and privileged. From the comfort of their
privilege, this elite prizes paternalism, as opposed to average
Americans who laud self-reliance and whose daily lives routinely demand
that they reckon with risk. That many of our leaders neglected to
consider the lived experience of those across the class divide is
unconscionable.
Incomprehensible to us due to this class divide,
we severely judged lockdown critics as lazy, backwards, even evil. We
dismissed as "grifters" those who represented their interests. We
believed "misinformation" energized the ignorant, and we refused to
accept that such people simply had a different, valid point of view.
We
crafted policy for the people without consulting them. If our public
health officials had led with less hubris, the course of the pandemic in
the United States might have had a very different outcome, with far
fewer lost lives.
My motivation for writing this is simple: It's clear to me that for
public trust to be restored in science, scientists should publicly
discuss what went right and what went wrong during the pandemic, and
where we could have done better.
It's OK to be wrong and admit
where one was wrong and what one learned. That's a central part of the
way science works. Yet I fear that many are too entrenched in
groupthink—and too afraid to publicly take responsibility—to do this.
Solving
these problems in the long term requires a greater commitment to
pluralism and tolerance in our institutions, including the inclusion of
critical if unpopular voices.
Intellectual elitism, credentialism, and classism must end. Restoring trust in public health—and our democracy—depends on it.
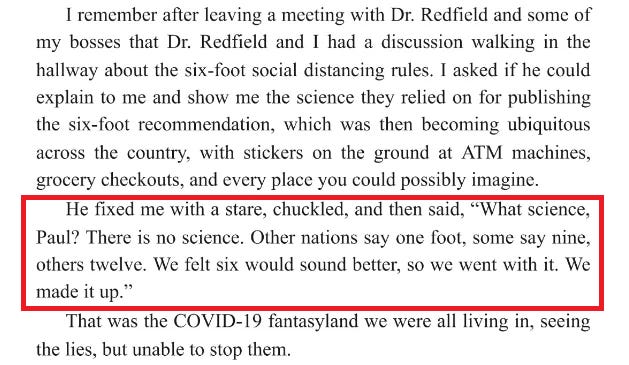
stevekirsch |Science used to be about data and what the data shows. Sadly, today, science is about what the CDC says, even if there is no data in support of the recommendation whatsoever.
The most stunning example of this is the “six foot rule.” Did you know that it was entirely fabricated out of thin air? From Presidential Takedown page 49:
What
is even more stunning is that the CDC has never admitted this publicly.
This is evidence that they are a corrupt organization and the
corruption goes to the very top of the organization.
We have over two years of data. Why not make it public?
We
now have over two years worth of death and vaccination data for people
who died after getting a COVID shot, yet nobody wants to see the record
level data tied to the vaccination dates?!?!
Let me be perfectly clear:
This is an abject failure of the entire medical community for not demanding to see this data.
People paid for us to see this data with their lives. Why is it being hidden from us?
In the US, hundreds of millions of people participated in a massive clinical trial and have data to share with people. At
least 500,000 of the participants paid the ultimate price: they
sacrificed their lives to send a message to America about the vaccines.
It is extremely disrespectful to these people to ignore their death
data and not share it with the public. Why are we not allowing these
people to share their data?
Do you think if we could ask
those people right before they died, “Do you want to let others know
what killed you?” Do you think they would all say, “No! Don’t let anyone
know. Please keep it a secret!”?
Every
institution in the world that is recommending or requiring COVID
vaccination should be DEMANDING to see this data made public
John Beaudoin and I have been calling for the death data to be set free and made public. We have been ignored.
Why aren’t any of these organizations calling for data transparency here so we can learn the truth?
The mainstream medical community
Heads of state throughout the world
The CDC
The FDA
The White House
Congress
The mainstream media
Public health authorities
Any doctor or nurse who recommends the jab to patients
Universities who mandate the vaccines for students, staff, or faculty
Any organization that supports COVID vaccines for their members, employees, or visitors
The data exists in VSD as well. But the CDC won’t allow anyone to see it.
The
data exists in every state health department. But you can’t FOIA it
because it requires a join to avoid PII problems and FOIA requests are
not allowed if they generate effort like that. So FOIA requests won’t
work.
It’s time for everyone to demand that our health authorities “Show us the data!”
We should all refuse to comply until they produce it.
brianoshea | Project Veritas recently released a video featuring "Jordon Trishton Walker," Pfizer executive who revealed shocking new info. But finding anything about him is tough. Here is what I've found so far.
thedailybeast |The Daily Mail took down a digital article last week that promoted Project Veritas’ latest sting operation
alleging that a Pfizer executive admitted the pharmaceutical giant was
making a “more potent” version of COVID in order to create new vaccines
for sale.
Following days of anti-vaxxers and right-wing media outlets
complaining about the article’s quiet deletion, and hours after The
Daily Beast reached out to the tabloid, the piece was back online—and
was completely changed.
Senior reporter Andrea Cavallier, the
article’s original author, was originally removed from the byline but
has since reappeared. The updated article,
which came back online Monday afternoon, now largely focuses on
Pfizer’s response to Project Veritas’ video and the far-right activist
group’s suggestion that the company is practicing “gain-of-function”
research. In addition to Cavallier, the byline now features health
editor Connor Boyd and health reporter Caitlin Tilley.
“Our
original story did not carry a response from Pfizer. We temporarily took
the story down while we vigorously pursued answers,” a Daily Mail
spokesperson told Confider. “Now Pfizer has responded, we are able to
report that they have confirmed they manipulated the covid
virus—although they insist there was no gain of function. This updated
story is now fully live again.”
In a video that went viral
in right-wing social media circles, a person Project Veritas claims is
Pfizer’s director of research and development tells an undercover
journalist that the company is “exploring” the possibility of “mutating”
viruses in monkeys so as to “preemptively develop new vaccines.”
“You’re
not supposed to do gain-of-function research with viruses,” the man,
whom Project Veritas claims is named Jordon Trishton Walker, added.
“Regularly not. We can do these selected structure mutations to make
them more potent. There is research ongoing about that. I don't know how
that is going to work. There better not be any more outbreaks because
Jesus Christ.”
The video blew up among conservatives, especially vaccine skeptics. Fox News’ Tucker Carlson fumed
about the “near-total media blackout of this story” about how Pfizer
was conducting “Frankenstein science.” GOP lawmakers soon began sending letters
to the company’s CEO asking him to confirm whether Pfizer was taking
part in gain-of-function research, citing Project Veritas’
“investigative report.” (Conservatives have latched onto
the theory that Dr. Anthony Fauci funded gain-of-function research in
Wuhan, largely blaming the “lab leak theory” for possibly creating
COVID-19.)
The Mail’s initial piece on the video
essentially gives a play-by-play of Project Veritas’ video while noting
the outlet reached out to Pfizer for comment. Shortly after it went up
on Thursday, however, the article was nowhere to be found on the
website. And its disappearance soon drew notice.
“Hi, @MailOnline
can you clarify why you have appeared to remove this story from your
website?” British parliament member Andrew Bridgen tweeted on Thursday. Bridgen was recently suspended by his own Conservative Party for peddling conspiracy theories about vaccines and comparing the side effects of COVID shots to the Holocaust.
After the Mail
piece was pulled offline, Pfizer released an online statement
responding to the allegations made about the company following the
publication of Project Veritas’ video.
“In the ongoing development
of the Pfizer-BioNTech COVID-19 vaccine, Pfizer has not conducted gain
of function or directed evolution research,” the statement, released Friday night,
said. “Working with collaborators, we have conducted research where the
original SARS-CoV-2 virus has been used to express the spike protein
from new variants of concern.”
The statement also added that “in a
limited number of cases when a full virus does not contain any known
gain of function mutations, such virus may be engineered to enable the
assessment of antiviral activity in cells.” The Mail’supdated article, which went back up on Monday afternoon, now largely focuses on Pfizer’s response to the undercover video.
A Foundation of Joy
-
Two years and I've lost count of how many times my eye has been operated
on, either beating the fuck out of the tumor, or reattaching that slippery
eel ...
April Three
-
4/3
43
When 1 = A and 26 = Z
March = 43
What day?
4 to the power of 3 is 64
64th day is March 5
My birthday
March also has 5 letters.
4 x 3 = 12
...
Return of the Magi
-
Lately, the Holy Spirit is in the air. Emotional energy is swirling out of
the earth.I can feel it bubbling up, effervescing and evaporating around
us, s...
New Travels
-
Haven’t published on the Blog in quite a while. I at least part have been
immersed in the area of writing books. My focus is on Science Fiction an
Historic...
Covid-19 Preys Upon The Elderly And The Obese
-
sciencemag | This spring, after days of flulike symptoms and fever, a man
arrived at the emergency room at the University of Vermont Medical Center.
He ...